

Outcome of 177Lu-PSMA-617 Radioligand Therapy in Chemo-Refractory Patients with Metastatic Castration-Resistant Early-Onset Prostate Cancer
- PMID: 34439347
- PMCID: PMC8392017
- DOI: 10.3390/cancers13164193
Outcome of 177Lu-PSMA-617 Radioligand Therapy in Chemo-Refractory Patients with Metastatic Castration-Resistant Early-Onset Prostate Cancer
Abstract
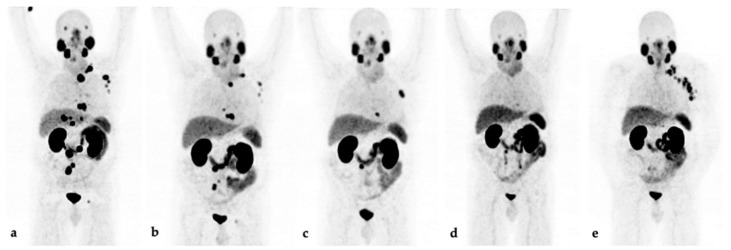
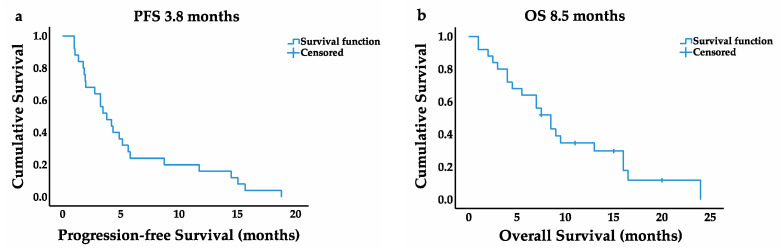
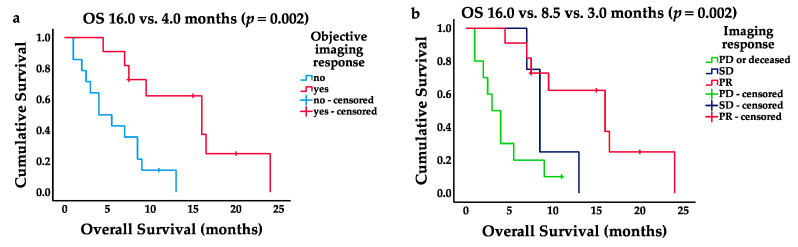
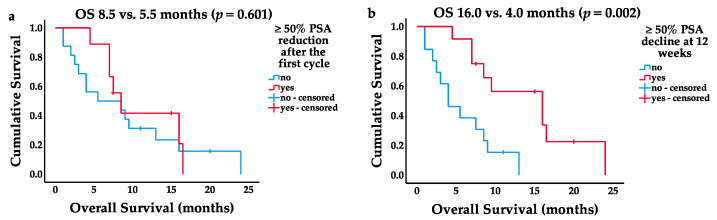
The aim of this retrospective study was to assess the outcome of patients with metastasized castration-resistant early-onset prostate cancer refractory to chemotherapy receiving radioligand therapy with 177Lutetium-PSMA-617 (LuPSMA-RLT). Twenty-five patients of ≤55 years of age at prostate cancer diagnosis, treated with a median of four (IQR 2-6) cycles (mean of 7.7 ± 1.4 GBq per cycle) every 6-8 weeks, were analyzed. Survival outcome was calculated based on the Kaplan-Meier method. The median progression-free survival (PFS) was 3.8 months (95% CI 2.3-5.3), and overall survival (OS) was 8.5 months (95% CI 6.2-10.8). An initial PSA reduction (≥ 50%) was observed in 9/25 (36%) of patients without being significantly associated with OS (p = 0.601). PSA response (PSA decline ≥50% at 12 weeks) was observed in 12/25 (48%) of patients and significantly associated with longer OS (16.0 months, 95% CI 7.4-24.6 vs. 4.0 months, 95% CI 1.1-6.9, p = 0.002). Imaging-based response using 68Ga-PSMA-11-PET/CT after two to three cycles was seen in 11/25 (44%). Additionally, responders had a significantly longer median PFS (8.7 months, 95% CI 1.3-16.1 vs. 1.9 months, 95% CI 1.7-2.2, p < 0.001) and OS (16.0 months, 95% CI 7.6-24.4 vs. 4.0 months, 95% CI 0.9-7.1; p = 0.002). Intra- or post-therapeutic toxicity was graded according to the CTCAE v5.0 criteria. Newly developing grade ≥ 3 anemia, leukopenia, and thrombocytopenia occurred in three (12%), one (4%), and three (12%) patients, respectively. One patient showed renal toxicity (grade ≥ 3) during follow-up. Pain palliation (>2 level VAS decline) was achieved in 9/14 (64%) and performance status improvement (ECOG level decline ≥ 1) in 8/17 (47%) of patients. Compared to previous reports, radioligand therapy with 177Lu-PSMA-617 in metastasized castration-resistant early-onset prostate cancer patients refractory to chemotherapy yields similar response rates with a comparable safety profile, but is associated with shorter survival.
Keywords: 177Lu-PSMA-617; PSMA; early-onset prostate cancer; metastatic castration-resistant prostate cancer; younger.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
