

Native Low-Density Lipoproteins Act in Synergy with Lipopolysaccharide to Alter the Balance of Human Monocyte Subsets and Their Ability to Produce IL-1 Beta, CCR2, and CX3CR1 In Vitro and In Vivo: Implications in Atherogenesis
- PMID: 34439835
- PMCID: PMC8391227
- DOI: 10.3390/biom11081169
Native Low-Density Lipoproteins Act in Synergy with Lipopolysaccharide to Alter the Balance of Human Monocyte Subsets and Their Ability to Produce IL-1 Beta, CCR2, and CX3CR1 In Vitro and In Vivo: Implications in Atherogenesis
Abstract
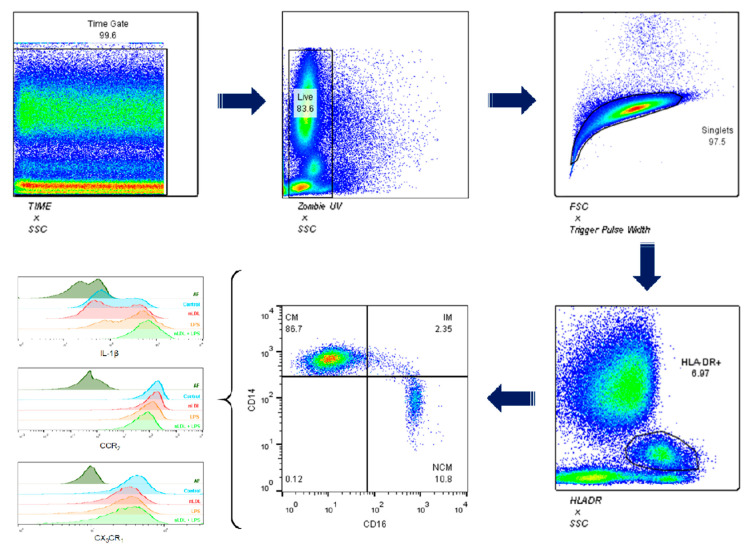
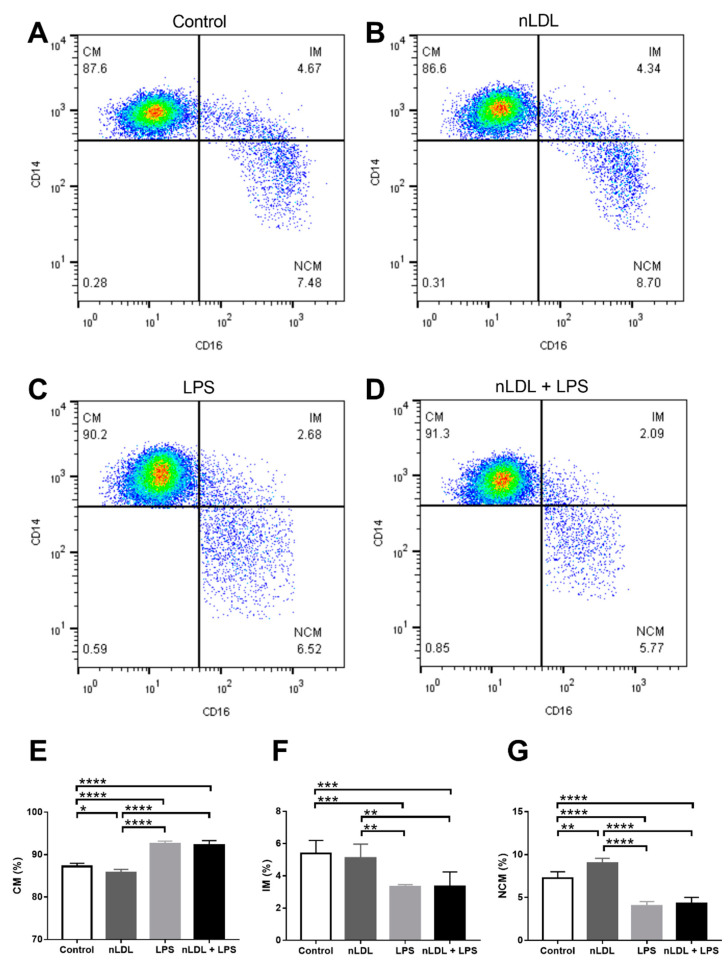
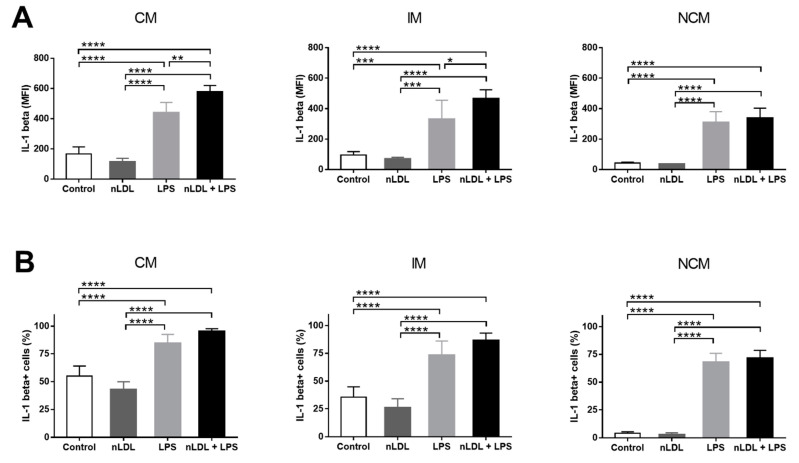
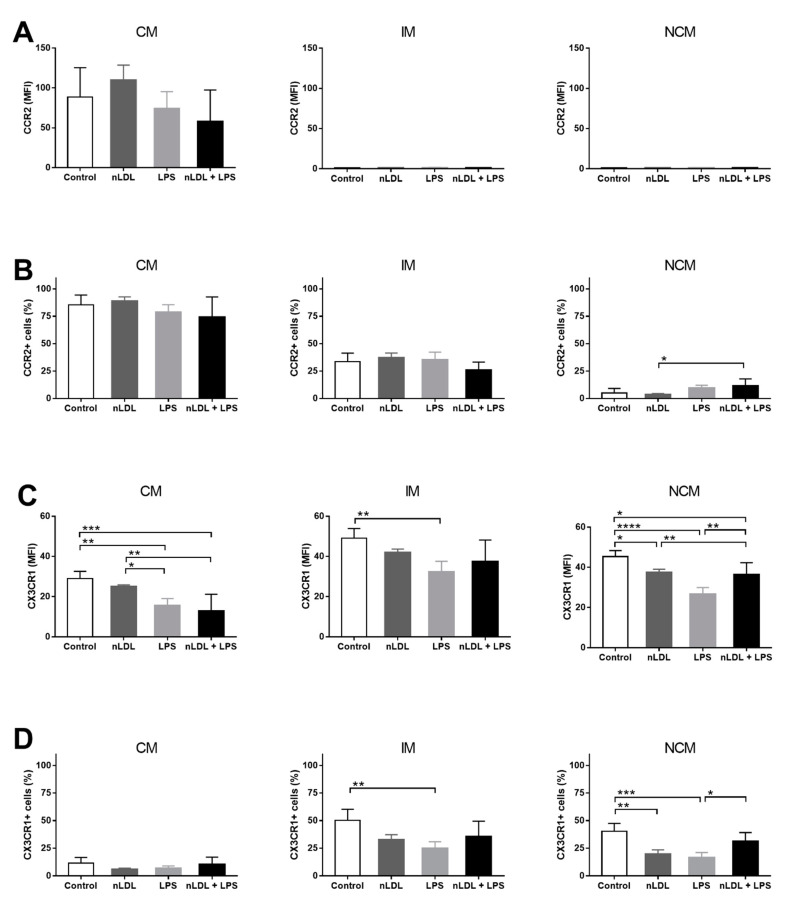
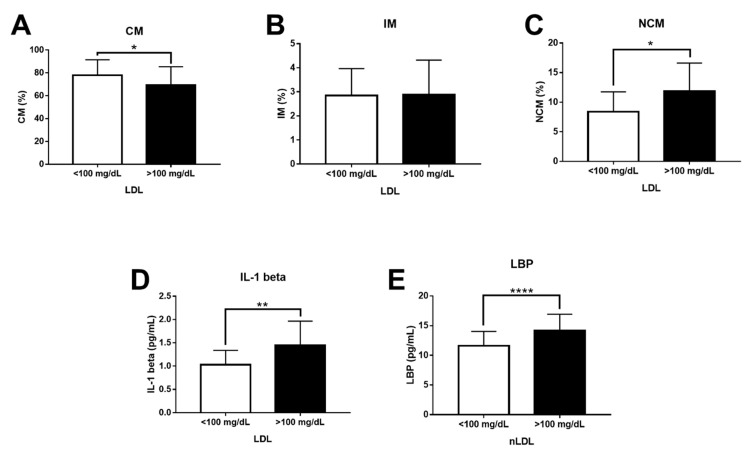
Increasing evidence has demonstrated that oxidized low-density lipoproteins (oxLDL) and lipopolysaccharide (LPS) enhance accumulation of interleukin (IL)-1 beta-producing macrophages in atherosclerotic lesions. However, the potential synergistic effect of native LDL (nLDL) and LPS on the inflammatory ability and migration pattern of monocyte subpopulations remains elusive and is examined here. In vitro, whole blood cells from healthy donors (n = 20) were incubated with 100 μg/mL nLDL, 10 ng/mL LPS, or nLDL + LPS for 9 h. Flow cytometry assays revealed that nLDL significantly decreases the classical monocyte (CM) percentage and increases the non-classical monocyte (NCM) subset. While nLDL + LPS significantly increased the number of NCMs expressing IL-1 beta and the C-C chemokine receptor type 2 (CCR2), the amount of NCMs expressing the CX3C chemokine receptor 1 (CX3CR1) decreased. In vivo, patients (n = 85) with serum LDL-cholesterol (LDL-C) >100 mg/dL showed an increase in NCM, IL-1 beta, LPS-binding protein (LBP), and Castelli's atherogenic risk index as compared to controls (n = 65) with optimal LDL-C concentrations (≤100 mg/dL). This work demonstrates for the first time that nLDL acts in synergy with LPS to alter the balance of human monocyte subsets and their ability to produce inflammatory cytokines and chemokine receptors with prominent roles in atherogenesis.
Keywords: CCR2; CX3CR1; IL-1 beta; LBP; LPS; atherogenesis; monocyte subpopulations; native LDL.
Conflict of interest statement
The authors declare no conflict of interest regarding the publication of this article.
Figures
References
-
- Song P., Fang Z., Wang H., Cai Y., Rahimi K., Zhu Y., Fowkes F.G.R., Fowkes F.J.I., Rudan I. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: A systematic review, meta-analysis, and modelling study. Lancet Glob. Health. 2020;8:e721–e729. doi: 10.1016/S2214-109X(20)30117-0. - DOI - PubMed
-
- Ganesan R., Henkels K.M., Wrenshall L.E., Kanaho Y., Di Paolo G., Frohman M.A., Gomez-Cambronero J. Oxidized LDL phagocytosis during foam cell formation in atherosclerotic plaques relies on a PLD2-CD36 functional interdependence. J. Leukoc. Biol. 2018;103:867–883. doi: 10.1002/JLB.2A1017-407RR. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
