

The Rise of SARS-CoV-2 Variants and the Role of Convalescent Plasma Therapy for Management of Infections
- PMID: 34440478
- PMCID: PMC8399171
- DOI: 10.3390/life11080734
The Rise of SARS-CoV-2 Variants and the Role of Convalescent Plasma Therapy for Management of Infections
Abstract
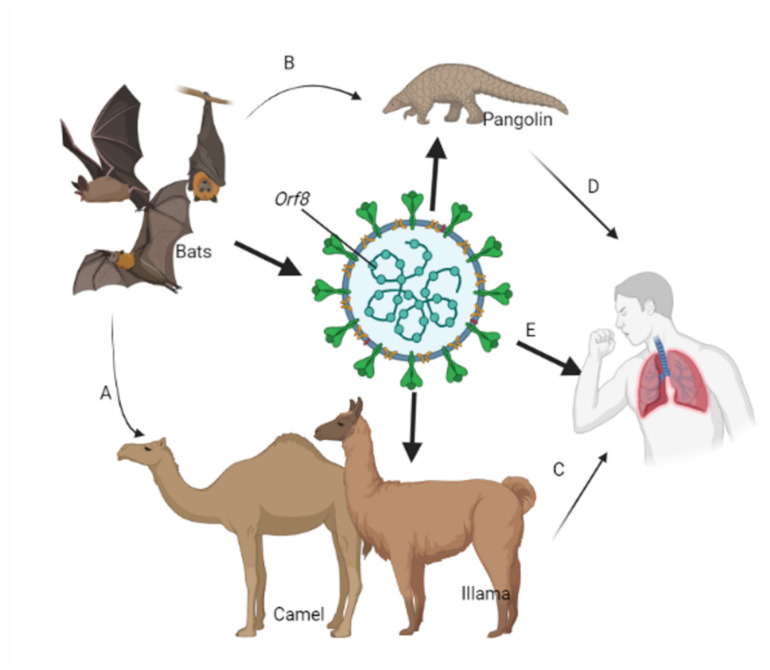
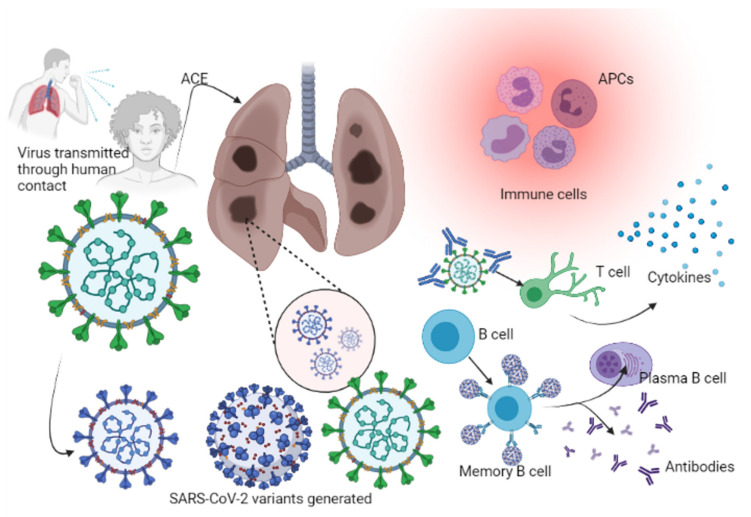
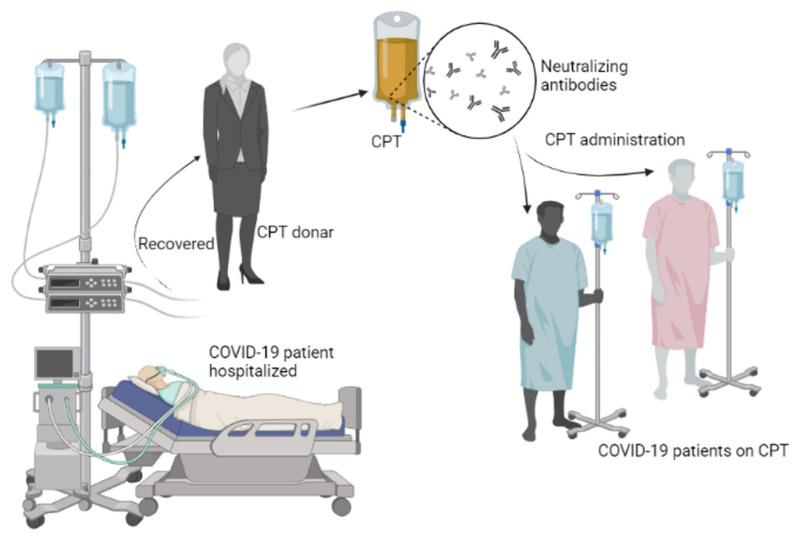
Novel therapies for the treatment of COVID-19 are continuing to emerge as the SARS-Cov-2 pandemic progresses. PCR remains the standard benchmark for initial diagnosis of COVID-19 infection, while advances in immunological profiling are guiding clinical treatment. The SARS-Cov-2 virus has undergone multiple mutations since its emergence in 2019, resulting in changes in virulence that have impacted on disease severity globally. The emergence of more virulent variants of SARS-Cov-2 remains challenging for effective disease control during this pandemic. Major variants identified to date include B.1.1.7, B.1.351; P.1; B.1.617.2; B.1.427; P.2; P.3; B.1.525; and C.37. Globally, large unvaccinated populations increase the risk of more and more variants arising. With successive waves of COVID-19 emerging, strategies that mitigate against community transmission need to be implemented, including increased vaccination coverage. For treatment, convalescent plasma therapy, successfully deployed during recent Ebola outbreaks and for H1N1 influenza, can increase survival rates and improve host responses to viral challenge. Convalescent plasma is rich with cytokines (IL-1β, IL-2, IL-6, IL-17, and IL-8), CCL2, and TNFα, neutralizing antibodies, and clotting factors essential for the management of SARS-CoV-2 infection. Clinical trials can inform and guide treatment policy, leading to mainstream adoption of convalescent therapy. This review examines the limited number of clinical trials published, to date that have deployed this therapy and explores clinical trials in progress for the treatment of COVID-19.
Keywords: COVID-19 convalescent therapy; COVID-19 therapy; COVID-19 vaccine; Ebola; SARS-CoV-2 infection; coronavirus; human antibodies; variants of concern.
Conflict of interest statement
The authors declare no conflict of interests exist.
Figures
References
-
- Monto A.S., Cowling B., Peiris J.S.M. Coronaviruses. Viral Infect. Hum. Epidemiol. Control. 2014:199–223. doi: 10.1007/978-1-4899-7448-8_10. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
