

Association between Cone-Beam Computed Tomography and Histological and Immunohistochemical Features in Periapical Lesions Correlated with Thickened Maxillary Sinus Mucosa
- PMID: 34441046
- PMCID: PMC8401138
- DOI: 10.3390/medicina57080840
Association between Cone-Beam Computed Tomography and Histological and Immunohistochemical Features in Periapical Lesions Correlated with Thickened Maxillary Sinus Mucosa
Abstract
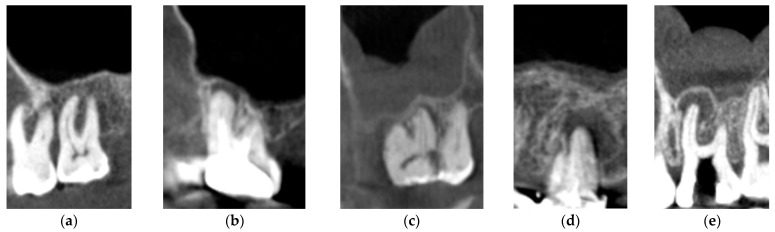
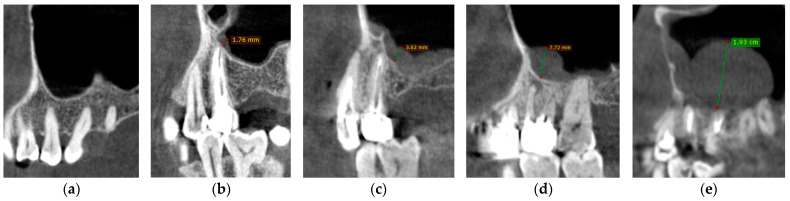
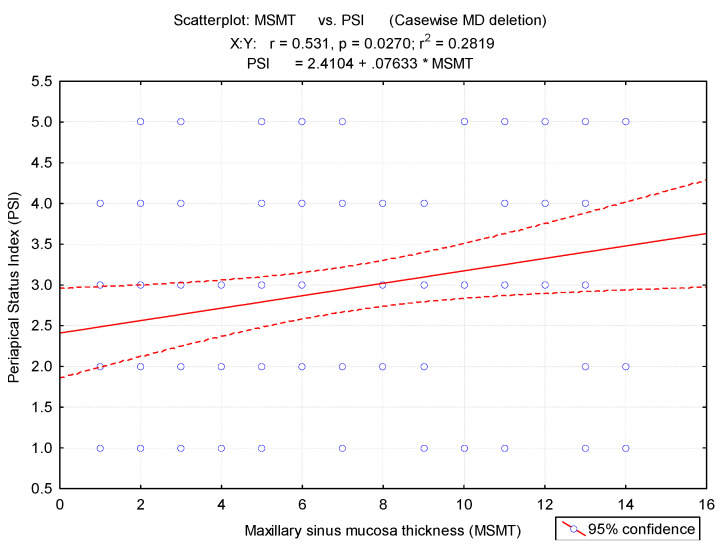
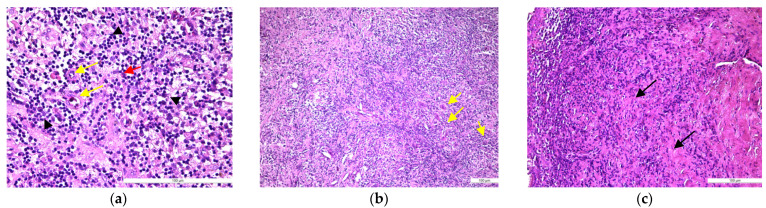
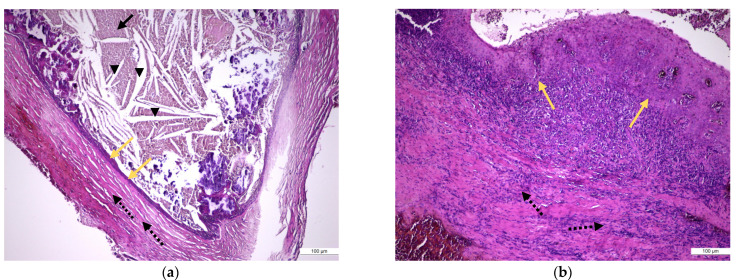
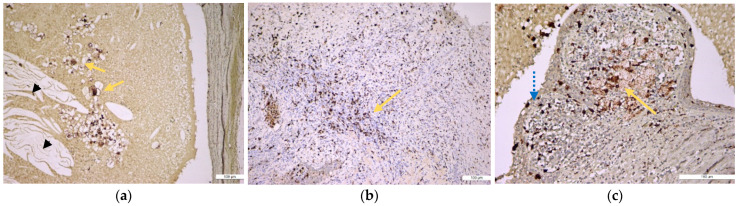
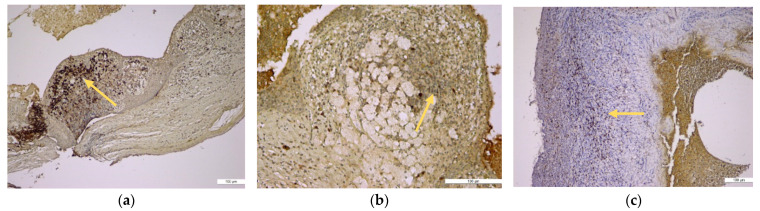
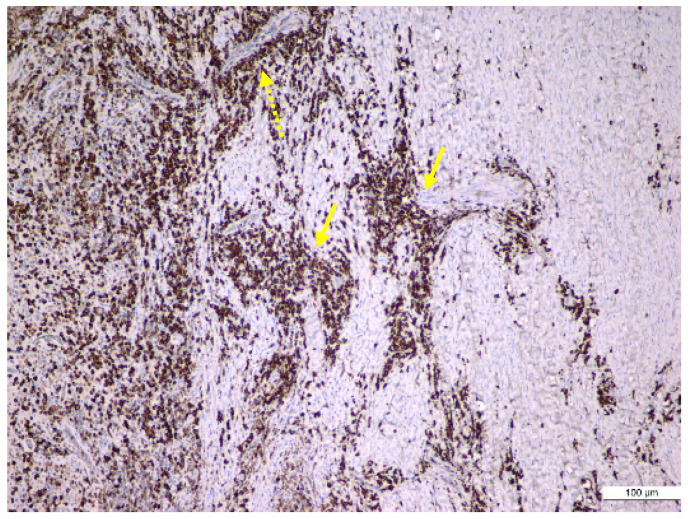
Background and Objectives: Odontogenic sinusitis is a frequently underestimated pathology with fewer symptoms in patients with periapical lesions, periodontal disease, or iatrogenic foreign bodies in the maxillary sinus. The aim of our study was to determine the correlation between maxillary sinusitis and periapical lesions using cone-beam computed tomography (CBCT) imaging and histological and immunohistochemical investigations. Materials and Methods: A total of 1450 initial patients diagnosed with maxillary sinusitis in the Ear-Nose-Throat (ENT) Department, University of Medicine and Pharmacy "Grigore T. Popa" Iasi, Romania, were treated with anti-inflammatory drugs. Of these, 629 still had unresolved symptomatology and were later referred to the Dental Medicine departments for further investigations. Only 50 subjects with periapical lesions in the premolar/molar maxillary area were included in the present study. All the periapical lesions were observed on CBCT and classified using the Periapical Status Index (PSI) and the mean maxillary sinus mucosa thicknesses (MSMT). The enrolled patients underwent surgical procedures with the excision of periapical lesions. The excised samples were submitted to the histological and immunohistochemical investigations. Results: The 50 patients presented periapical lesions of their maxillary teeth in 328 dental units. There was a higher prevalence of periapical lesions in men than in women (chi-square test). We observed a significant difference between the mean MSMT of individuals with periapical lesions compared to those without (p < 0.01). Mean MSMT was 1.23 mm for teeth without periapical lesions and 3.95 mm for teeth with periapical lesions. The histopathological study identified 50% cases with periapical granulomas, 10% cases with periapical granulomas with cystic potential, and 40% cases as periapical cysts. Immunohistochemical stainings showed that CD4+ helper and CD8+ cytotoxic T lymphocytes, along with CD20+ B lymphocytes and CD68+ macrophages, were diffusely distributed in all periapical cysts and in some periapical granulomas, but CD79α+ plasma cells characterized especially periapical granulomas. Conclusions: The current study observed a significant correlation between CBCT maxillary mucosa thickness and type of periapical lesion. Chronic inflammatory lympho-histiocytic infiltrate predominates in periapical lesions, supporting the idea that lesion progression is determined by a humoral-type (CD20+ and CD79α+ B lymphocytes) but also by a cellular-type (CD4+ and CD8+ T lymphocyte population) immune mechanism.
Keywords: cone-beam computed tomography; endo-perio lesions; immunohistochemistry; odontogenic sinusitis; periapical cyst; periapical granuloma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
