

Pulmonary Congestion Assessment in Heart Failure: Traditional and New Tools
- PMID: 34441241
- PMCID: PMC8394474
- DOI: 10.3390/diagnostics11081306
Pulmonary Congestion Assessment in Heart Failure: Traditional and New Tools
Abstract
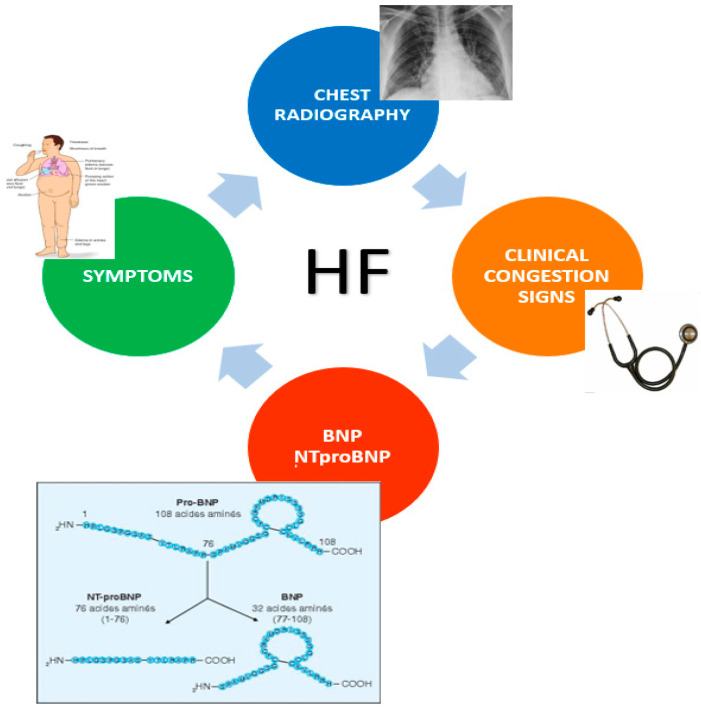
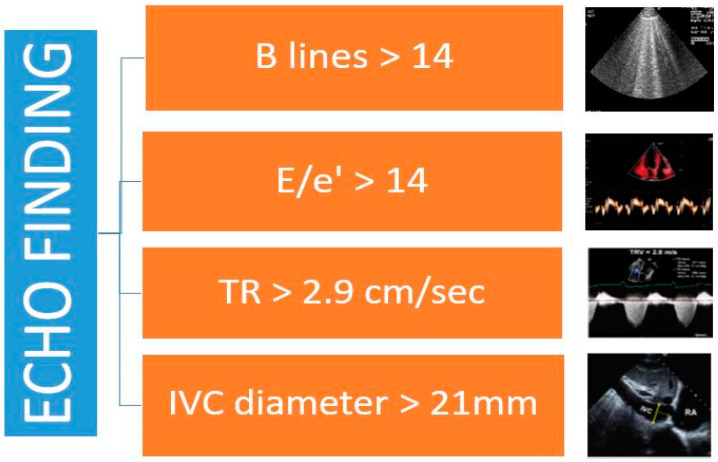
Congestion related to cardiac pressure and/or volume overload plays a central role in the pathophysiology, presentation, and prognosis of heart failure (HF). Most HF exacerbations are related to a progressive rise in cardiac filling pressures that precipitate pulmonary congestion and symptomatic decompensation. Furthermore, persistent symptoms and signs of congestion at discharge or among outpatients are strong predictors of an adverse outcome. Pulmonary congestion is also one of the most important diagnostic and therapeutic targets in chronic heart failure. The aim of this review is to analyze the importance of clinical, instrumental, and biochemical evaluation of congestion in HF by describing old and new tools. Lung ultrasonography (LUS) is an emerging method to assess pulmonary congestion. Accordingly, we describe the additive prognostic role of chest ultrasound with respect to traditional clinical and X-ray assessment in acute and chronic HF setting.
Keywords: clinical assessment; congestion; heart failure.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Mentz R.J., Stevens S.R., DeVore A.D., Lala A., Vader J.M., AbouEzzeddine O.F., Khazanie P., Redfield M.M., Stevenson L.W., O’Connor C.M., et al. Decongestion strategies and renin–angiotensin–aldosterone system activation in acute heart failure. JACC Heart Fail. 2015;3:97–107. doi: 10.1016/j.jchf.2014.09.003. - DOI - PMC - PubMed
-
- Ambrosy A.P., Pang P., Khan S., Konstam M.A., Fonarow G., Traver B., Maggioni A.P., Cook T., Swedberg K., Burnett J.C., et al. Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: Findings from the EVEREST trial. Eur. Heart J. 2013;34:835–843. doi: 10.1093/eurheartj/ehs444. - DOI - PubMed
-
- Volpicelli G., Elbarbary M., Blaivas M., Lichtenstein D.A., Mathis G., Kirkpatrick A.W., Melniker L., Gargani L., Noble V.E., International Liaison Committee on Lung Ultrasound (ILC-LUS) for the International Consensus Conference on Lung Ultrasound (ICC-LUS) et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensiv. Care Med. 2012;38:577–591. doi: 10.1007/s00134-012-2513-4. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
