

Clinical Management of Moyamoya Patients
- PMID: 34441923
- PMCID: PMC8397113
- DOI: 10.3390/jcm10163628
Clinical Management of Moyamoya Patients
Abstract
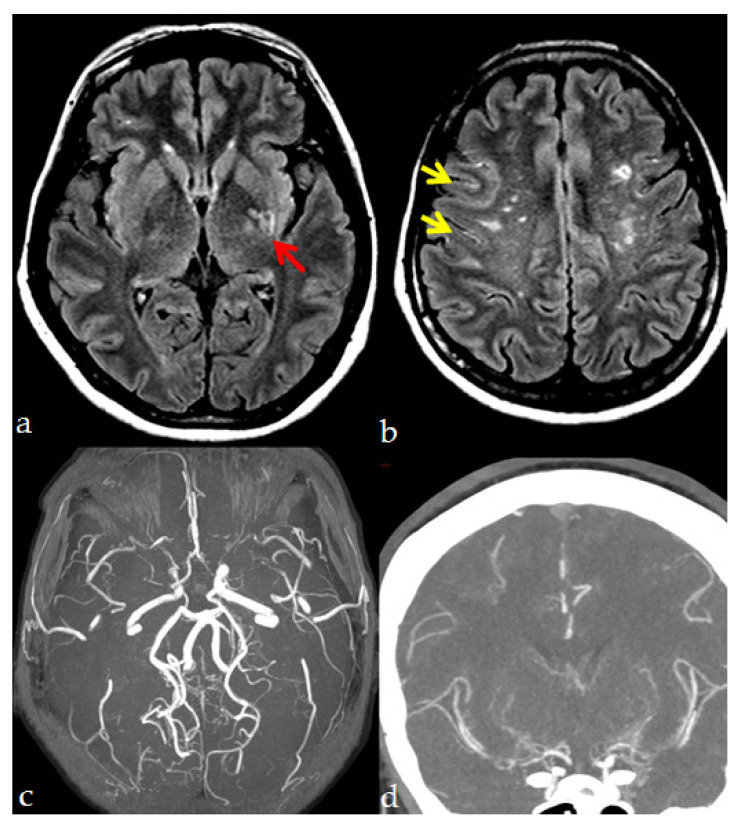
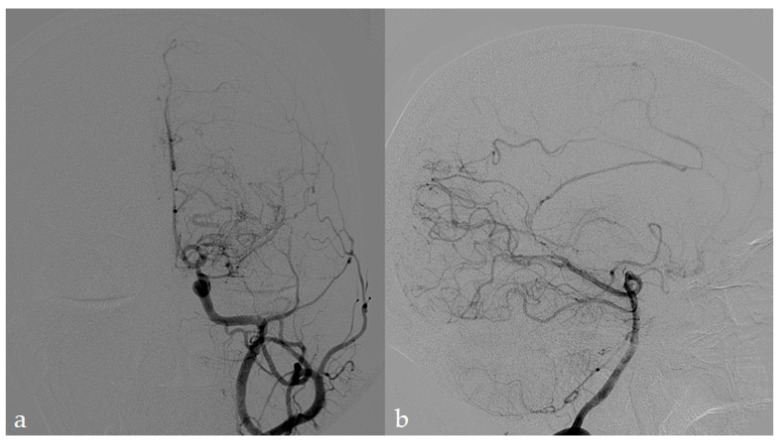
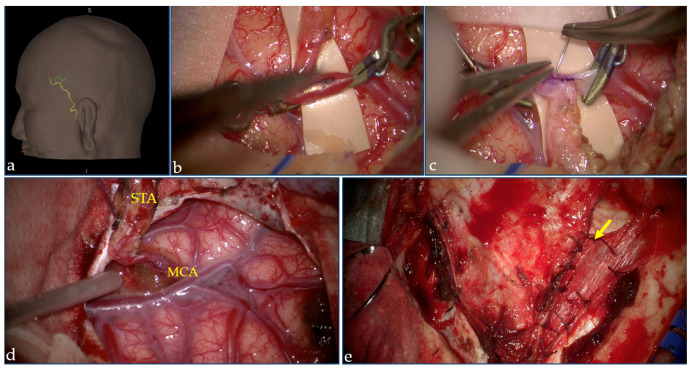
Moyamoya angiopathy (MMA) is a peculiar cerebrovascular condition characterized by progressive steno-occlusion of the terminal part of the internal carotid arteries (ICAs) and their proximal branches, associated with the development of a network of fragile collateral vessels at the base of the brain. The diagnosis is essentially made by radiological angiographic techniques. MMA is often idiopathic (moyamoya disease-MMD); conversely, it can be associated with acquired or hereditary conditions (moyamoya Syndrome-MMS); however, the pathophysiology underlying either MMD or MMS has not been fully elucidated to date, and this poor knowledge reflects uncertainties and heterogeneity in patient management. MMD and MMS also have similar clinical expressions, including, above all, ischemic and hemorrhagic strokes, then headaches, seizures, cognitive impairment, and movement disorders. The available treatment strategies are currently shared between idiopathic MMD and MMS, including pharmacological and surgical stroke prevention treatments and symptomatic drugs. No pharmacological treatment able to reverse the progressive disappearance of the ICAs has been found to date in both idiopathic and syndromic cases. Antithrombotic agents are usually prescribed in ischemic MMA, although the coexisting hemorrhagic risk should be considered. Surgical revascularization techniques, which are currently the best available treatment in symptomatic MMA, are associated with good long-term outcomes and reduced ischemic and hemorrhagic risks. Given the lack of dedicated randomized clinical trials, current treatment is mainly based on observational studies and physicians' and surgeons' expertise.
Keywords: diagnosis; management; moyamoya angiopathy; moyamoya disease; moyamoya syndrome; revascularization; therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Fukui M. Guidelines for the diagnosis and treatment of spontaneous occlusion of the circle of Willis (“moyamoya” disease). Research Committee on Spontaneous Occlusion of the Circle of Willis (Moyamoya Disease) of the Ministry of Health and Welfare, Japan. Clin. Neurol. Neurosurg. 1997;99(Suppl. 2):S238–S240. doi: 10.1016/S0303-8467(97)00082-6. - DOI - PubMed
