

GDF-15 Predicts In-Hospital Mortality of Critically Ill Patients with Acute Kidney Injury Requiring Continuous Renal Replacement Therapy: A Multicenter Prospective Study
- PMID: 34441955
- PMCID: PMC8397174
- DOI: 10.3390/jcm10163660
GDF-15 Predicts In-Hospital Mortality of Critically Ill Patients with Acute Kidney Injury Requiring Continuous Renal Replacement Therapy: A Multicenter Prospective Study
Abstract
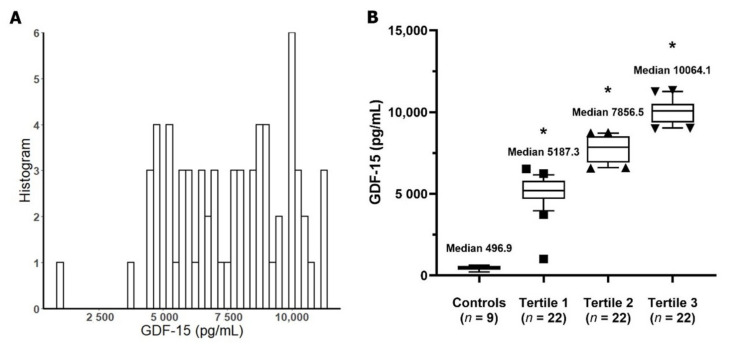
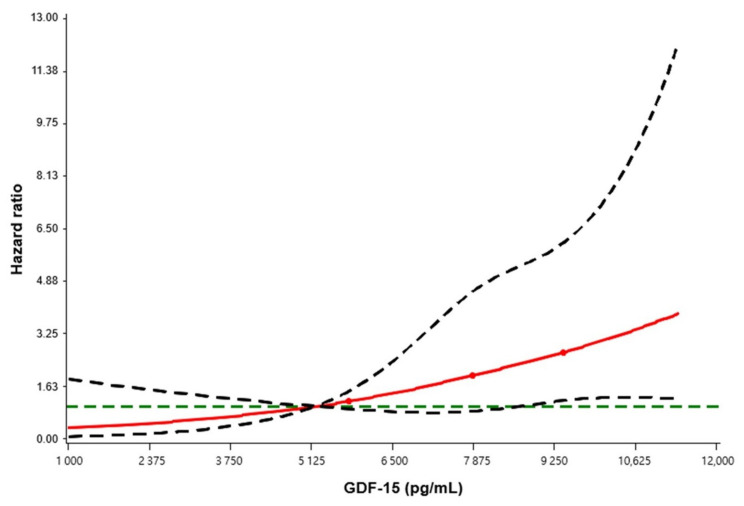
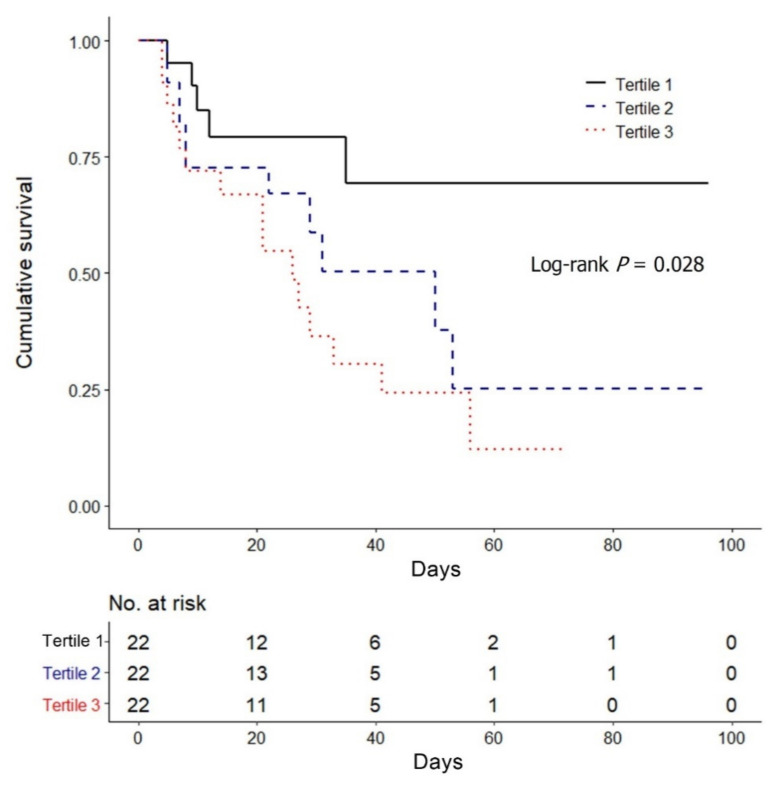
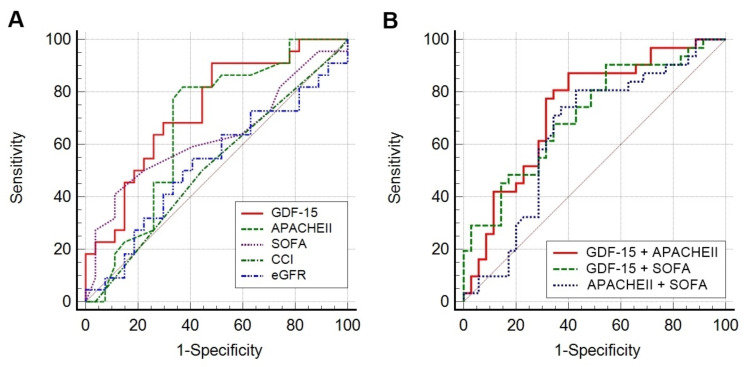
Growth differentiation factor-15 (GDF-15) is a stress-responsive cytokine. This study evaluated the association between GDF-15 and in-hospital mortality among patients with severe acute kidney injury (AKI) requiring continuous renal replacement therapy (CRRT). Among the multicenter prospective CRRT cohort between 2017 and 2019, 66 patients whose blood sample was available were analyzed. Patients were divided into three groups according to the GDF-15 concentrations. The median GDF-15 level was 7865.5 pg/mL (496.9 pg/mL in the healthy control patients). Baseline characteristics were not different among tertile groups except the severity scores and serum lactate level, which were higher in the third tertile. After adjusting for confounding factors, the patients with higher GDF-15 had significantly increased risk of mortality (second tertile: adjusted hazards ratio [aHR], 3.67; 95% confidence interval [CI], 1.05-12.76; p = 0.041; third tertile: aHR, 6.81; 95% CI, 1.98-23.44; p = 0.002). Furthermore, GDF-15 predicted in-hospital mortality (area under the curve, 0.710; 95% CI, 0.585-0.815) better than APACHE II and SOFA scores. Serum GDF-15 concentration was elevated in AKI patients requiring CRRT, higher in more severe patients. GDF-15 is a better independent predictor for in-hospital mortality of critically ill AKI patients than the traditional risk scoring system such as APACHE II and SOFA scores.
Keywords: acute kidney injury; continuous renal replacement therapy; growth differentiation factor-15; in-hospital mortality.
Conflict of interest statement
All authors declared no conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
