

Clinical Evaluation of Different Treatment Strategies for Motor Recovery in Poststroke Rehabilitation during the First 90 Days
- PMID: 34442014
- PMCID: PMC8396898
- DOI: 10.3390/jcm10163718
Clinical Evaluation of Different Treatment Strategies for Motor Recovery in Poststroke Rehabilitation during the First 90 Days
Abstract
Background: Motor recovery after stroke is based on neuronal plasticity and the structural reorganization of the brain. Questions are debated about the proper moment to start rehabilitation in the acute period of stroke, the significance of rehabilitation interventions during the so-called "plastic window", and the advantages of modern and traditional programs. The aims of this study were to evaluate the role of different rehabilitation strategies and their combinations for motor recovery and the impact on functional disability by way of neurological and functional outcomes 3 months after ischemic stroke.
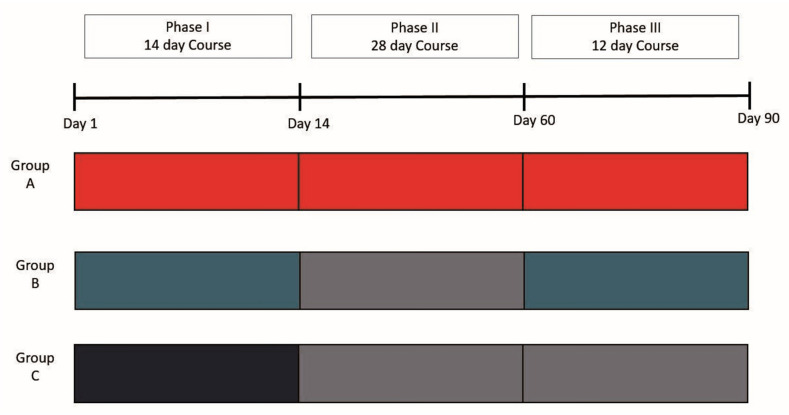
Methods: We used three rehabilitation approaches: early rehabilitation from the first day of stroke (Phase I), traditional exercise programs (Phase II), and an author's new method of biofeedback rehabilitation using motion sensors and augmented reality (AR) rehabilitation (Phase III). Clinical and functional outcomes were measured on the 90th day after stroke. We developed algorithms for quantifying the quality of movements during the execution of tasks in the motor domains of the AR rehabilitation program.
Results: Phase I of rehabilitation led to an improvement in functional independence, and the recovery of motor functions of the extremities with an absence of mortality and clinical deterioration. AR rehabilitation led to significant improvement both with respect to clinical and functional scores on scales and to variables reflecting the quality of movements. Patients who were actively treated during Phases II and III achieved the same final level of motor recovery and functional outcomes as that of participants who had only received AR rehabilitation during Phase III. Patients who underwent outpatient observation after Phase I showed a deficit of spontaneous motor recovery on the 90th day after stroke.
Conclusions: Early rehabilitation was successful but was not enough; rehabilitation programs should be carried out throughout the entire "sensitive period" of poststroke plasticity. The newly developed AR biofeedback motion training is effective and safe as a separate rehabilitation method in the early recovery period of moderately severe, hemiparalytic, and ischemic stroke. These two rehabilitation approaches must be applied together or after each other, not instead of each other, as shown in clinical practice.
Keywords: augmented reality rehabilitation; clinical and functional outcomes; early recovery period; ischemic stroke; motor recovery; movement assessment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Serum BDNF's Role as a Biomarker for Motor Training in the Context of AR-Based Rehabilitation after Ischemic Stroke.Brain Sci. 2020 Sep 9;10(9):623. doi: 10.3390/brainsci10090623. Brain Sci. 2020. PMID: 32916851 Free PMC article.
-
Construction of efficacious gait and upper limb functional interventions based on brain plasticity evidence and model-based measures for stroke patients.ScientificWorldJournal. 2007 Dec 20;7:2031-45. doi: 10.1100/tsw.2007.299. ScientificWorldJournal. 2007. PMID: 18167618 Free PMC article.
-
Assessing functional recovery in the first six months after acute ischemic stroke: a prospective, observational study.Eur J Phys Rehabil Med. 2019 Feb;55(1):1-7. doi: 10.23736/S1973-9087.18.05161-4. Epub 2018 May 14. Eur J Phys Rehabil Med. 2019. PMID: 29764094
-
Motor learning: its relevance to stroke recovery and neurorehabilitation.Curr Opin Neurol. 2006 Feb;19(1):84-90. doi: 10.1097/01.wco.0000200544.29915.cc. Curr Opin Neurol. 2006. PMID: 16415682 Review.
-
Stroke Rehabilitation.Continuum (Minneap Minn). 2017 Feb;23(1, Cerebrovascular Disease):238-253. doi: 10.1212/CON.0000000000000423. Continuum (Minneap Minn). 2017. PMID: 28157752 Review.
Cited by
-
Acceptability, Feasibility, and Effectiveness of Immersive Virtual Technologies to Promote Exercise in Older Adults: A Systematic Review and Meta-Analysis.Sensors (Basel). 2023 Feb 24;23(5):2506. doi: 10.3390/s23052506. Sensors (Basel). 2023. PMID: 36904709 Free PMC article.
-
Serum BDNF's Role as a Biomarker for Motor Training in the Context of AR-Based Rehabilitation after Ischemic Stroke.Brain Sci. 2020 Sep 9;10(9):623. doi: 10.3390/brainsci10090623. Brain Sci. 2020. PMID: 32916851 Free PMC article.
-
A Wearable Mixed Reality Platform to Augment Overground Walking: A Feasibility Study.Front Hum Neurosci. 2022 Jun 9;16:868074. doi: 10.3389/fnhum.2022.868074. eCollection 2022. Front Hum Neurosci. 2022. PMID: 35754777 Free PMC article.
-
Emerging Applications of Augmented and Mixed Reality Technologies in Motor Rehabilitation: A Scoping Review.Sensors (Basel). 2025 Mar 25;25(7):2042. doi: 10.3390/s25072042. Sensors (Basel). 2025. PMID: 40218554 Free PMC article.
-
Customized Manual Muscle Testing for Post-Stroke Upper Extremity Assessment.Brain Sci. 2022 Mar 28;12(4):457. doi: 10.3390/brainsci12040457. Brain Sci. 2022. PMID: 35447988 Free PMC article.
References
-
- Hatem S.M., Saussez G., Della Faille M., Prist V., Zhang X., Dispa D., Bleyenheuft Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016;10:442. doi: 10.3389/fnhum.2016.00442. - DOI - PMC - PubMed
-
- Feigin V.L., Forouzanfar M.H., Krishnamurthi R., Mensah G.A., Connor M., Bennett D.A., Moran A.E., Sacco R.L., Anderson L., Truelsen T., et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet. 2013;383:245–255. doi: 10.1016/S0140-6736(13)61953-4. - DOI - PMC - PubMed
-
- Feigin V.L., Krishnamurthi R.V., Parmar P., Norrving B., Mensah G.A., Bennett D.A., Barker-Collo S., Moran A.E., Sacco R.L., Truelsen T., et al. Update on the Global Burden of Ischemic and Hemorrhagic Stroke in 1990-2013: The GBD 2013 Study. Neuroepidemiology. 2015;45:161–176. doi: 10.1159/000441085. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
