

Multi-Drug Resistance Bacterial Infections in Critically Ill Patients Admitted with COVID-19
- PMID: 34442852
- PMCID: PMC8402127
- DOI: 10.3390/microorganisms9081773
Multi-Drug Resistance Bacterial Infections in Critically Ill Patients Admitted with COVID-19
Abstract
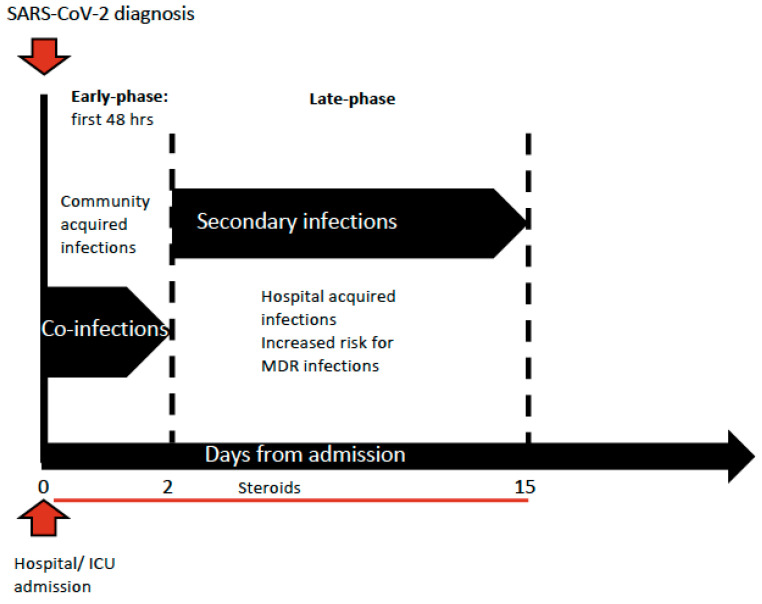
It is known that bacterial infections represent a common complication during viral respiratory tract infections such as influenza, with a concomitant increase in morbidity and mortality. Nevertheless, the prevalence of bacterial co-infections and secondary infections in critically ill patients affected by coronavirus disease 2019 (COVID-19) is not well understood yet. We performed a review of the literature currently available to examine the incidence of bacterial secondary infections acquired during hospital stay and the risk factors associated with multidrug resistance. Most of the studies, mainly retrospective and single-centered, highlighted that the incidence of co-infections is low, affecting about 3.5% of hospitalized patients, while the majority are hospital acquired infections, developed later, generally 10-15 days after ICU admission. The prolonged ICU hospitalization and the extensive use of broad-spectrum antimicrobial drugs during the COVID-19 outbreak might have contributed to the selection of pathogens with different profiles of resistance. Consequently, the reported incidence of MDR bacterial infections in critically ill COVID-19 patients is high, ranging between 32% to 50%. MDR infections are linked to a higher length of stay in ICU but not to a higher risk of death. The only risk factor independently associated with MDR secondary infections reported was invasive mechanical ventilation (OR 1.062; 95% CI 1.012-1.114), but also steroid therapy and prolonged length of ICU stay may play a pivotal role. The empiric antimicrobial therapy for a ventilated patient with suspected or proven bacterial co-infection at ICU admission should be prescribed judiciously and managed according to a stewardship program in order to interrupt or adjust it on the basis of culture results.
Keywords: COVID-19; SARS-CoV-2; critically ill patients; hospital acquired infection; multi-drug resistance; secondary bacterial infections.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Rice T.W., Rubinson L., Uyeki T.M., Vaughn F.L., John B.B., Miller R.R., 3rd, Higgs E., Randolph A.G., Smoot B.E., Thompson B.T., et al. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States. Crit. Care Med. 2012;40:1487–1498. doi: 10.1097/CCM.0b013e3182416f23. - DOI - PMC - PubMed
-
- Shah N.S., Greenberg J.A., McNulty M.C., Gregg K.S., Riddell J.t., Mangino J.E., Weber D.M., Hebert C.L., Marzec N.S., Barron M.A., et al. Bacterial and viral co-infections complicating severe influenza: Incidence and impact among 507 U.S. patients, 2013–2014. J. Clin. Virol. 2016;80:12–19. doi: 10.1016/j.jcv.2016.04.008. - DOI - PMC - PubMed
-
- Martin-Loeches I., Sanchez-Corral A., Diaz E., Granada R.M., Zaragoza R., Villavicencio C., Albaya A., Cerda E., Catalan R.M., Luque P., et al. Community-acquired respiratory coinfection in critically ill patients with pandemic 2009 influenza A(H1N1) virus. Chest. 2011;139:555–562. doi: 10.1378/chest.10-1396. - DOI - PubMed
-
- Alhazzani W., Moller M.H., Arabi Y.M., Loeb M., Gong M.N., Fan E., Oczkowski S., Levy M.M., Derde L., Dzierba A., et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19) Intensive Care Med. 2020;46:854–887. doi: 10.1007/s00134-020-06022-5. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
