

Patient-Derived Organoids of Cholangiocarcinoma
- PMID: 34445380
- PMCID: PMC8395494
- DOI: 10.3390/ijms22168675
Patient-Derived Organoids of Cholangiocarcinoma
Abstract
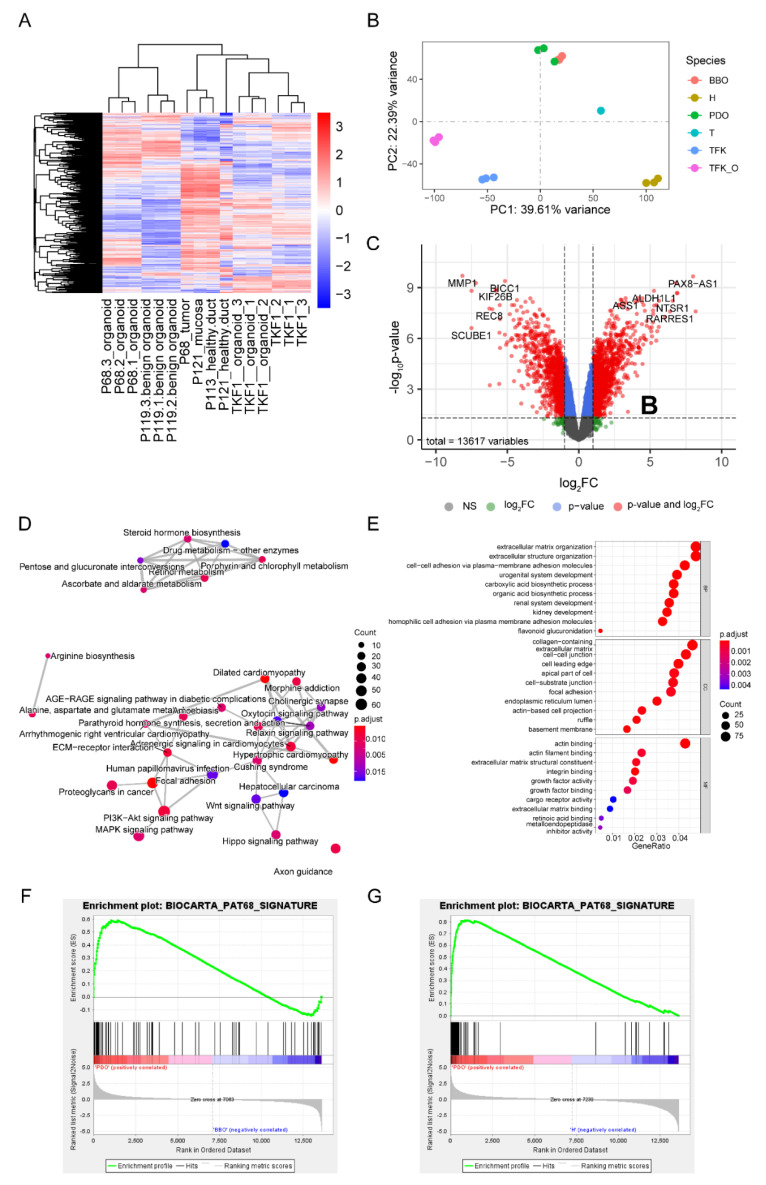
Cholangiocarcinoma (CC) is an aggressive malignancy with an inferior prognosis due to limited systemic treatment options. As preclinical models such as CC cell lines are extremely rare, this manuscript reports a protocol of cholangiocarcinoma patient-derived organoid culture as well as a protocol for the transition of 3D organoid lines to 2D cell lines. Tissue samples of non-cancer bile duct and cholangiocarcinoma were obtained during surgical resection. Organoid lines were generated following a standardized protocol. 2D cell lines were generated from established organoid lines following a novel protocol. Subcutaneous and orthotopic patient-derived xenografts were generated from CC organoid lines, histologically examined, and treated using standard CC protocols. Therapeutic responses of organoids and 2D cell lines were examined using standard CC agents. Next-generation exome and RNA sequencing was performed on primary tumors and CC organoid lines. Patient-derived organoids closely recapitulated the original features of the primary tumors on multiple levels. Treatment experiments demonstrated that patient-derived organoids of cholangiocarcinoma and organoid-derived xenografts can be used for the evaluation of novel treatments and may therefore be used in personalized oncology approaches. In summary, this study establishes cholangiocarcinoma organoids and organoid-derived cell lines, thus expanding translational research resources of cholangiocarcinoma.
Keywords: cholangiocarcinoma; next-generation sequencing; organoids; orthotopic xenograft; patient-derived organoids; precision medicine; response prediction; translational surgical oncology; xenograft model.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
