

Initial antimicrobial management of sepsis
- PMID: 34446092
- PMCID: PMC8390082
- DOI: 10.1186/s13054-021-03736-w
Initial antimicrobial management of sepsis
Abstract
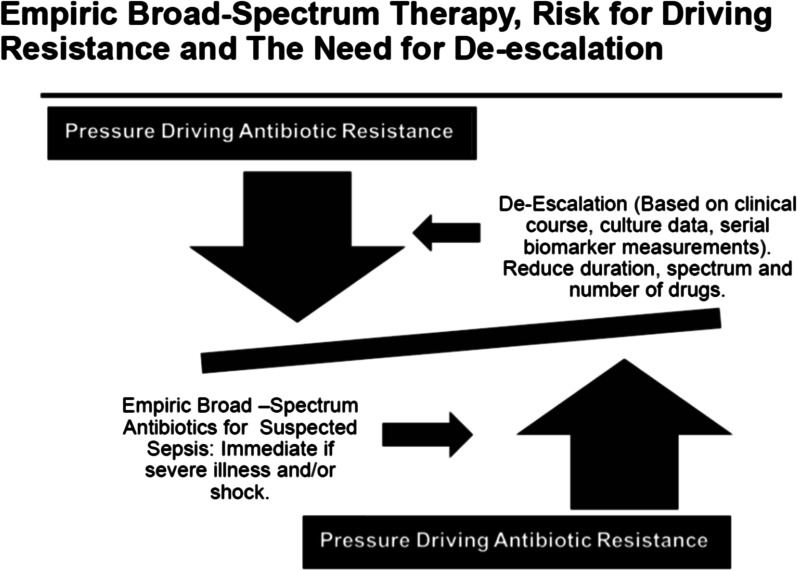
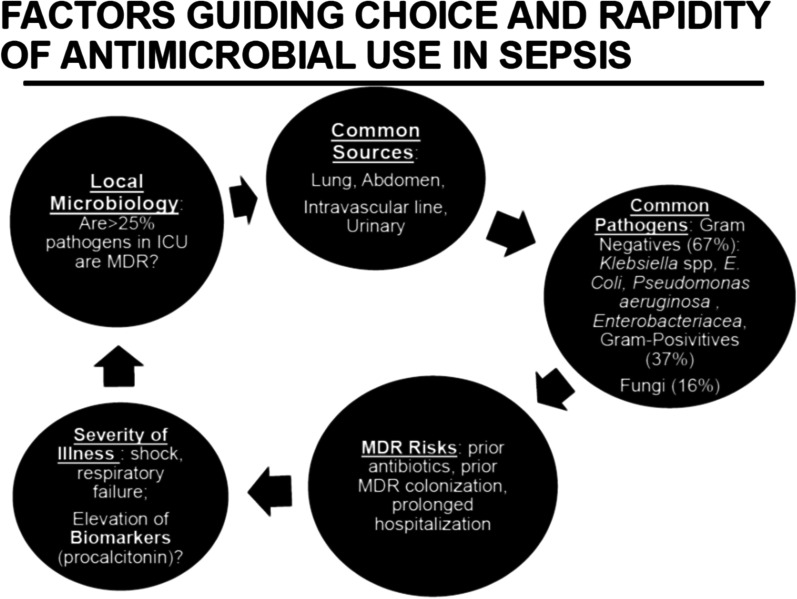
Sepsis is a common consequence of infection, associated with a mortality rate > 25%. Although community-acquired sepsis is more common, hospital-acquired infection is more lethal. The most common site of infection is the lung, followed by abdominal infection, catheter-associated blood steam infection and urinary tract infection. Gram-negative sepsis is more common than gram-positive infection, but sepsis can also be due to fungal and viral pathogens. To reduce mortality, it is necessary to give immediate, empiric, broad-spectrum therapy to those with severe sepsis and/or shock, but this approach can drive antimicrobial overuse and resistance and should be accompanied by a commitment to de-escalation and antimicrobial stewardship. Biomarkers such a procalcitonin can provide decision support for antibiotic use, and may identify patients with a low likelihood of infection, and in some settings, can guide duration of antibiotic therapy. Sepsis can involve drug-resistant pathogens, and this often necessitates consideration of newer antimicrobial agents.
Keywords: Antibiotic therapy; Antimicrobial therapy; Bacteremia; Biomarkers; Fungal infection; Intra-abdominal infection; Pharmacokinetics; Pneumonia; Sepsis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Initial antimicrobial management of sepsis: increased prehospital blood lactate levels for identifying sicker patients who may benefit from prehospital antibiotic therapy initiation.Crit Care. 2021 Oct 30;25(1):377. doi: 10.1186/s13054-021-03801-4. Crit Care. 2021. PMID: 34717739 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
