

Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study
- PMID: 34446426
- PMCID: PMC8388189
- DOI: 10.1136/bmj.n1931
Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study
Abstract
Objective: To assess the association between covid-19 vaccines and risk of thrombocytopenia and thromboembolic events in England among adults.
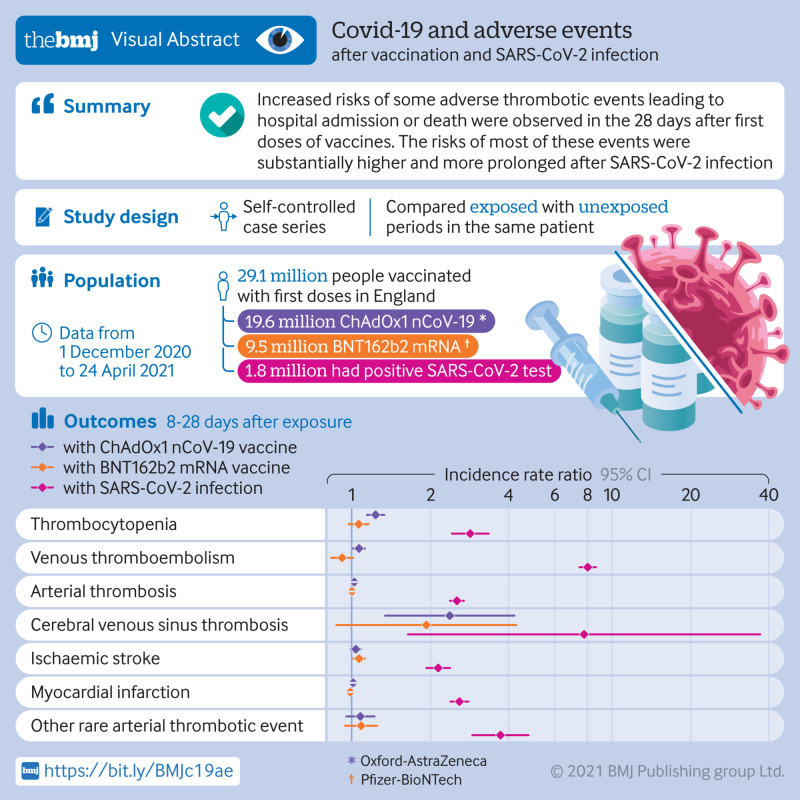
Design: Self-controlled case series study using national data on covid-19 vaccination and hospital admissions.
Setting: Patient level data were obtained for approximately 30 million people vaccinated in England between 1 December 2020 and 24 April 2021. Electronic health records were linked with death data from the Office for National Statistics, SARS-CoV-2 positive test data, and hospital admission data from the United Kingdom's health service (NHS).
Participants: 29 121 633 people were vaccinated with first doses (19 608 008 with Oxford-AstraZeneca (ChAdOx1 nCoV-19) and 9 513 625 with Pfizer-BioNTech (BNT162b2 mRNA)) and 1 758 095 people had a positive SARS-CoV-2 test. People aged ≥16 years who had first doses of the ChAdOx1 nCoV-19 or BNT162b2 mRNA vaccines and any outcome of interest were included in the study.
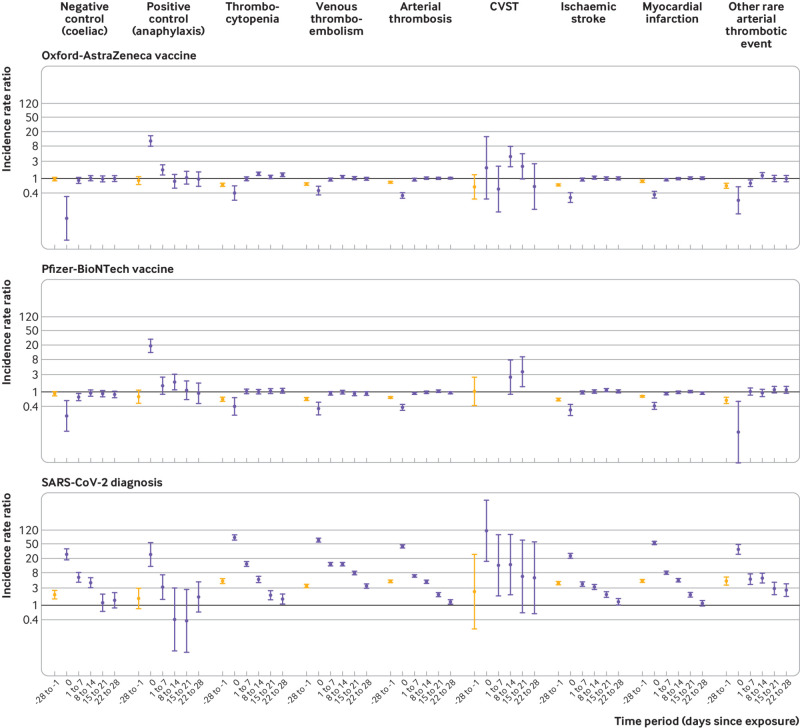
Main outcome measures: The primary outcomes were hospital admission or death associated with thrombocytopenia, venous thromboembolism, and arterial thromboembolism within 28 days of three exposures: first dose of the ChAdOx1 nCoV-19 vaccine; first dose of the BNT162b2 mRNA vaccine; and a SARS-CoV-2 positive test. Secondary outcomes were subsets of the primary outcomes: cerebral venous sinus thrombosis (CVST), ischaemic stroke, myocardial infarction, and other rare arterial thrombotic events.
Results: The study found increased risk of thrombocytopenia after ChAdOx1 nCoV-19 vaccination (incidence rate ratio 1.33, 95% confidence interval 1.19 to 1.47 at 8-14 days) and after a positive SARS-CoV-2 test (5.27, 4.34 to 6.40 at 8-14 days); increased risk of venous thromboembolism after ChAdOx1 nCoV-19 vaccination (1.10, 1.02 to 1.18 at 8-14 days) and after SARS-CoV-2 infection (13.86, 12.76 to 15.05 at 8-14 days); and increased risk of arterial thromboembolism after BNT162b2 mRNA vaccination (1.06, 1.01 to 1.10 at 15-21 days) and after SARS-CoV-2 infection (2.02, 1.82 to 2.24 at 15-21 days). Secondary analyses found increased risk of CVST after ChAdOx1 nCoV-19 vaccination (4.01, 2.08 to 7.71 at 8-14 days), after BNT162b2 mRNA vaccination (3.58, 1.39 to 9.27 at 15-21 days), and after a positive SARS-CoV-2 test; increased risk of ischaemic stroke after BNT162b2 mRNA vaccination (1.12, 1.04 to 1.20 at 15-21 days) and after a positive SARS-CoV-2 test; and increased risk of other rare arterial thrombotic events after ChAdOx1 nCoV-19 vaccination (1.21, 1.02 to 1.43 at 8-14 days) and after a positive SARS-CoV-2 test.
Conclusion: Increased risks of haematological and vascular events that led to hospital admission or death were observed for short time intervals after first doses of the ChAdOx1 nCoV-19 and BNT162b2 mRNA vaccines. The risks of most of these events were substantially higher and more prolonged after SARS-CoV-2 infection than after vaccination in the same population.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from UK Research and Innovation for the submitted work. JHC reports grants from the John Fell Oxford University Press Research Fund, Cancer Research UK (CR-UK) grant No C5255/A18085, through the Cancer Research UK Oxford Centre and the Oxford Wellcome Institutional Strategic Support Fund (204826/Z/16/Z) during the conduct of the study; JHC is an unpaid director of QResearch, a not-for-profit organisation, which is a partnership between the University of Oxford and EMIS Health who supply the QResearch database used for this work; JHC is a founder and shareholder of ClinRisk and was its medical director until 31 May 2019; JHC is member of the SAGE subgroups on ethnicity and data, and is chair of the risk stratification subgroup of NERVTAG (New and Emerging Respiratory Virus Threats Advisory Group). The views expressed are those of the authors only. AS is a member of the Scottish Government’s Chief Medical Officer’s COVID-19 Advisory Group and a member of AstraZeneca’s COVID-19 Strategic Consultancy Group: Thrombocytopenia Taskforce; both roles are unremunerated. PST reports previous consultations with AstraZeneca and Duke-NUS outside the submitted work. KK is member of the Scientific Advisory Group for Emergencies (SAGE) and Independent SAGE. SJG administers covid-19 vaccinations.
Figures
Comment in
-
Strengthening international surveillance of vaccine safety.BMJ. 2021 Aug 26;374:n1994. doi: 10.1136/bmj.n1994. BMJ. 2021. PMID: 34446436 No abstract available.
References
-
- The New York Times. Tracking coronavirus vaccinations around the world 2021. https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracke....
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous