

Establishing standardized immune phenotyping of metastatic melanoma by digital pathology
- PMID: 34446805
- PMCID: PMC8590976
- DOI: 10.1038/s41374-021-00653-y
Establishing standardized immune phenotyping of metastatic melanoma by digital pathology
Erratum in
-
Correction: Establishing standardized immune phenotyping of metastatic melanoma by digital pathology.Lab Invest. 2021 Dec;101(12):1637. doi: 10.1038/s41374-021-00676-5. Lab Invest. 2021. PMID: 34584200 Free PMC article. No abstract available.
Abstract
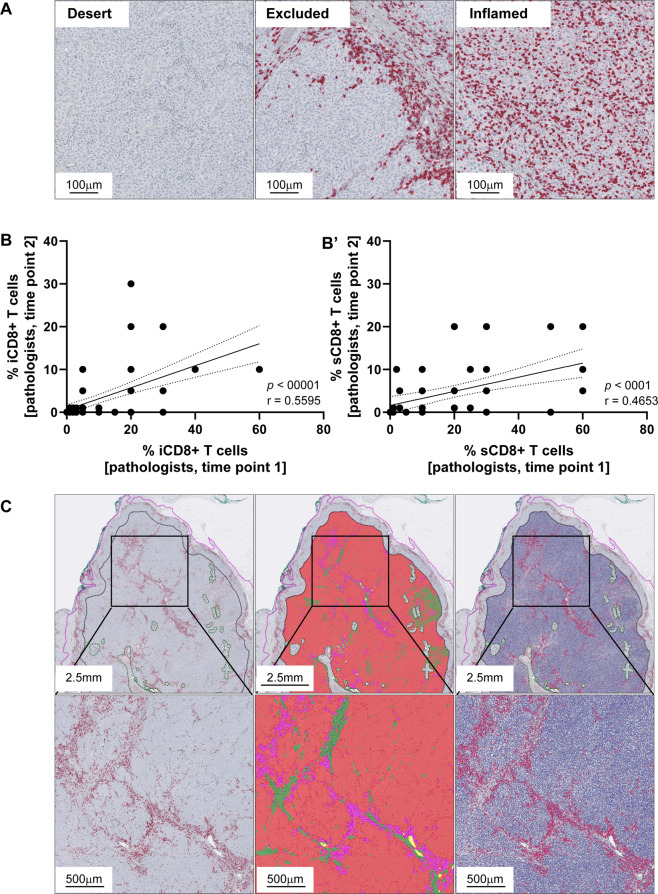
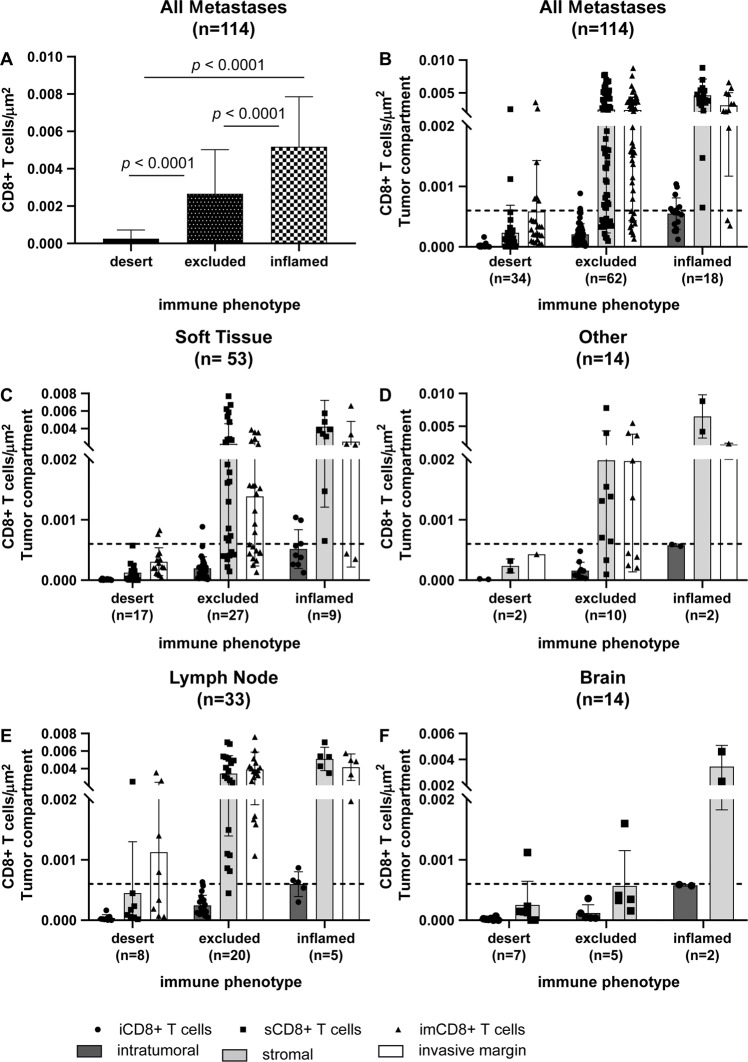
CD8+ tumor-infiltrating T cells can be regarded as one of the most relevant predictive biomarkers in immune-oncology. Highly infiltrated tumors, referred to as inflamed (clinically "hot"), show the most favorable response to immune checkpoint inhibitors in contrast to tumors with a scarce immune infiltrate called immune desert or excluded (clinically "cold"). Nevertheless, quantitative and reproducible methods examining their prevalence within tumors are lacking. We therefore established a computational diagnostic algorithm to quantitatively measure spatial densities of tumor-infiltrating CD8+ T cells by digital pathology within the three known tumor compartments as recommended by the International Immuno-Oncology Biomarker Working Group in 116 prospective metastatic melanomas of the Swiss Tumor Profiler cohort. Workflow robustness was confirmed in 33 samples of an independent retrospective validation cohort. The introduction of the intratumoral tumor center compartment proved to be most relevant for establishing an immune diagnosis in metastatic disease, independent of metastatic site. Cut-off values for reproducible classification were defined and successfully assigned densities into the respective immune diagnostic category in the validation cohort with high sensitivity, specificity, and precision. We provide a robust diagnostic algorithm based on intratumoral and stromal CD8+ T-cell densities in the tumor center compartment that translates spatial densities of tumor-infiltrating CD8+ T cells into the clinically relevant immune diagnostic categories "inflamed", "excluded", and "desert". The consideration of the intratumoral tumor center compartment allows immune phenotyping in the clinically highly relevant setting of metastatic lesions, even if the invasive margin compartment is not captured in biopsy material.
© 2021. The Author(s).
Conflict of interest statement
V.H.K. has served as an invited speaker on behalf of Indica Labs. H.M. is on advisory boards for Bayer, Astra Zeneca, Janssen, Roche, and Merck. R.D. reports intermittent, project-focused consulting and/or advisory relationships with Novartis, Merck Sharp & Dohme (MSD), Bristol Myers Squibb (BMS), Roche, Amgen, Takeda, Pierre Fabre, Sun Pharma, Sanofi, Catalym, Second Genome, Regeneron, and Alligator outside the submitted work. M.P.L. is a co-founder and shareholder of Oncobit AG and receives research funding from Novartis, Roche, and Molecular Partners. All other authors declare no conflict of interest.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
