

Incidence and predictors of delirium on the intensive care unit in patients with acute kidney injury, insight from a retrospective registry
- PMID: 34446816
- PMCID: PMC8390667
- DOI: 10.1038/s41598-021-96839-x
Incidence and predictors of delirium on the intensive care unit in patients with acute kidney injury, insight from a retrospective registry
Abstract
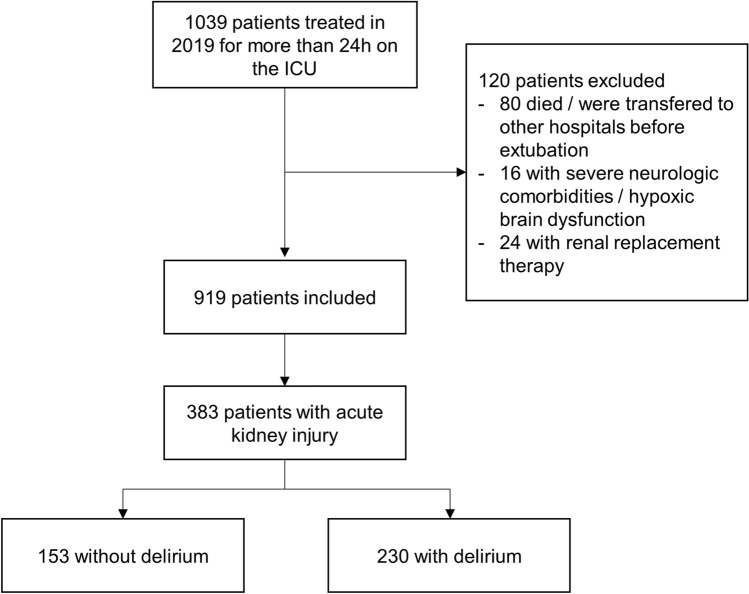
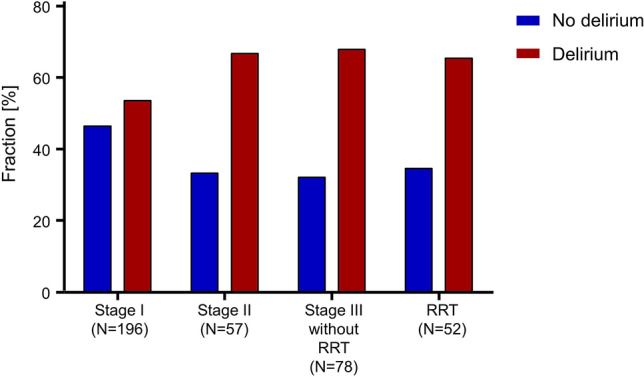
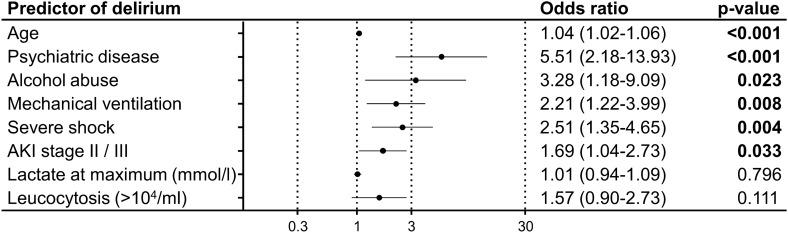
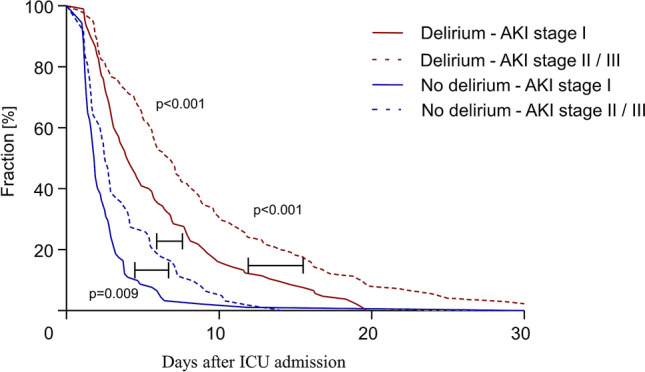
Acute kidney injury (AKI) and delirium are common complications on the intensive care unit (ICU). Few is known about the association of AKI and delirium, as well as about incidence and predictors of delirium in patients with AKI. In this retrospective study, all patients with AKI, as defined by the KDIGO (kidney disease improving global outcome) guideline, treated for more than 24 h on the ICU in an university hospital in 2019 were included and analyzed. Delirium was defined by a NuDesc (Nursing Delirium screening scale) ≥ 2, which is evaluated three times a day in every patient on our ICU as part of daily routine. A total of 383/919 (41.7%) patients developed an AKI during the ICU stay. Delirium was detected in 230/383 (60.1%) patients with AKI. Independent predictors of delirium were: age, psychiatric disease, alcohol abuse, mechanical ventilation, severe shock, and AKI stage II/III (all p < 0.05). The primary cause of illness had no influence on the onset of delirium. Among patients with AKI, the duration of the ICU stay correlated with higher stages of AKI and the presence of delirium (stage I/no delirium: median 1.9 (interquartile range (25th-75th) 1.3-2.9) days; stage II/III/no delirium: 2.6 (1.6-5.5) days; stage I/delirium: 4.1 (2.5-14.3) days; stage II/III/delirium: 6.8 (3.5-11.9) days; all p < 0.01). Delirium, defined as NuDesc ≥ 2 is frequent in patients with AKI on an ICU and independently predicted by higher stages of AKI.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- German Society of Anaesthesiology and Intensive Care Medicine (DGAI), German Interdisciplinary Association for Intensive Care and Emergency Medicine (DIVI). German S3 Guidelines. Analgesia, Sedation and Management of Delirium on the Intensive Care Unit (2015). https://www.awmf.org/leitlinien/detail/ll/001-012.html. Accessed 20 Dec 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
