

Triage Modeling for Differential Diagnosis Between COVID-19 and Human Influenza A Pneumonia: Classification and Regression Tree Analysis
- PMID: 34447759
- PMCID: PMC8382719
- DOI: 10.3389/fmed.2021.673253
Triage Modeling for Differential Diagnosis Between COVID-19 and Human Influenza A Pneumonia: Classification and Regression Tree Analysis
Abstract
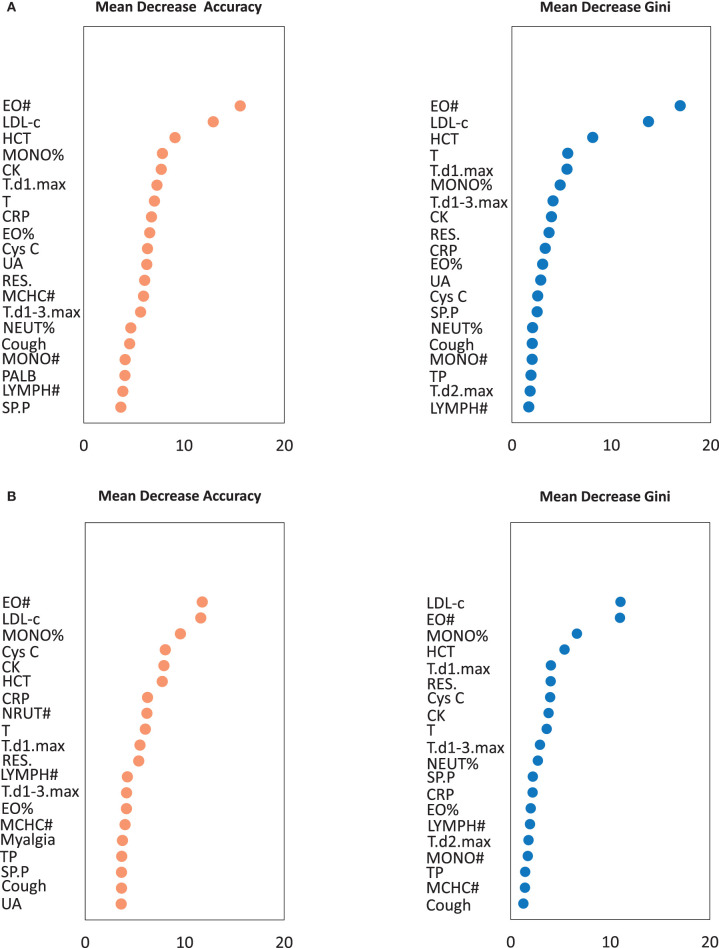
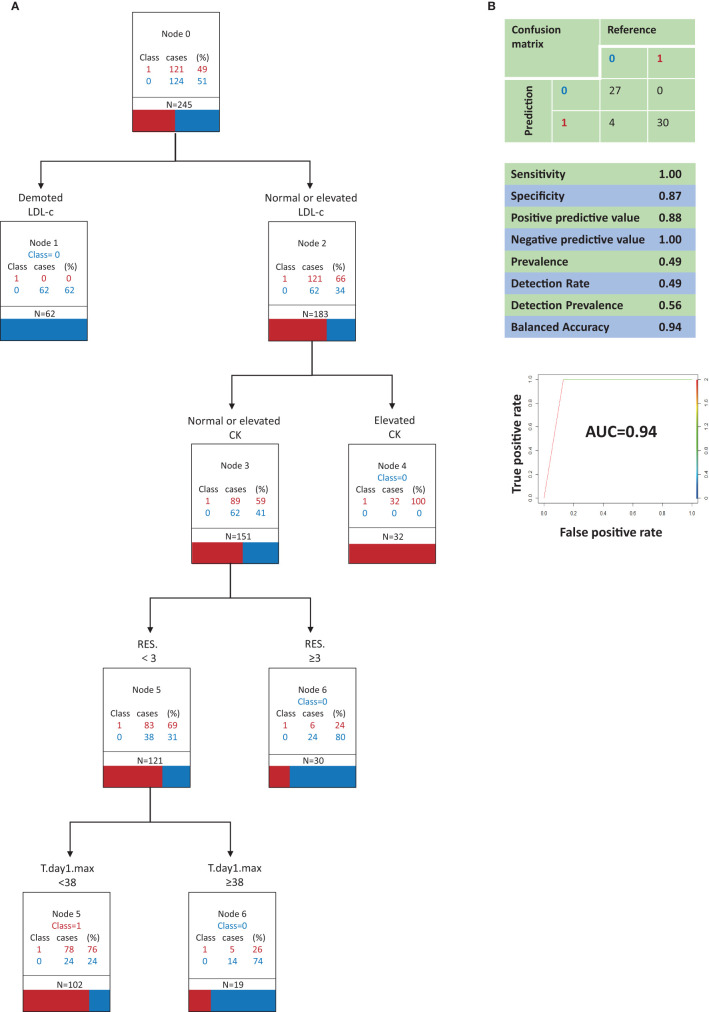
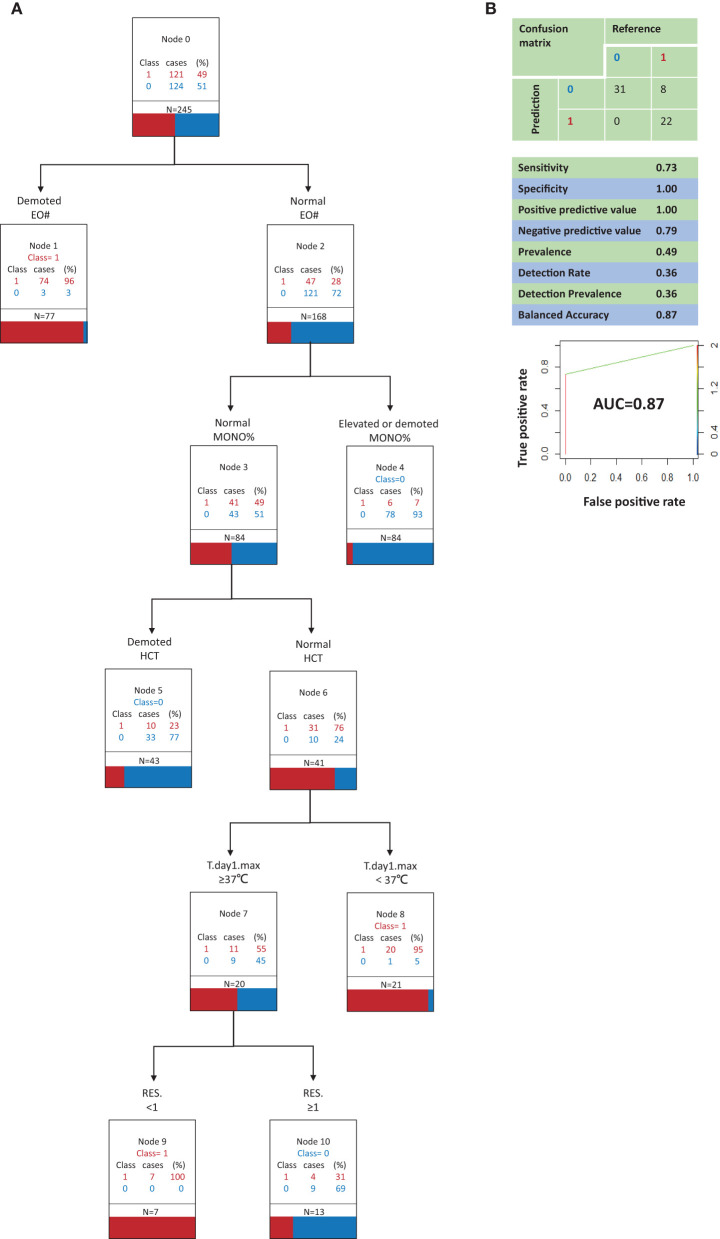
Background: The coronavirus disease 2019 (COVID-19) pandemic has lasted much longer than an influenza season, but the main signs, symptoms, and some imaging findings are similar in COVID-19 and influenza patients. The aim of the current study was to construct an accurate and robust model for initial screening and differential diagnosis of COVID-19 and influenza A. Methods: All patients in the study were diagnosed at Fuyang No. 2 People's Hospital, and they included 151 with COVID-19 and 155 with influenza A. The patients were randomly assigned to training set or a testing set at a 4:1 ratio. Predictor variables were selected based on importance, assessed by random forest algorithms, and analyzed to develop classification and regression tree models. Results: In the optimal model A, the best single predictor of COVID-19 patients was a normal or high level of low-density lipoprotein cholesterol, followed by low level of creatine kinase, then the presence of <3 respiratory symptoms, then a highest temperature on the first day of admission <38°C. In the suboptimal model B, the best single predictor of COVID-19 was a low eosinophil count, then a normal monocyte ratio, then a normal hematocrit value, then a highest temperature on the first day of admission of <37°C, then a complete lack of respiratory symptoms. Conclusions: The two models provide clinicians with a rapid triage tool. The optimal model can be used to developed countries/regions and major hospitals, and the suboptimal model can be used in underdeveloped regions and small hospitals.
Keywords: COVID-19; differential diagnosis; influenza A; rapid triage tools; regression tree analysis.
Copyright © 2021 Xiao, Zhao, Xia, Zhang, Zhang, Ruan, Mei, Li, Ma, Wang, He, Lee, Zhu, Tian, Zhang, Zheng and Yin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effects of short-term exposure to air pollution on hospital admissions of young children for acute lower respiratory infections in Ho Chi Minh City, Vietnam.Res Rep Health Eff Inst. 2012 Jun;(169):5-72; discussion 73-83. Res Rep Health Eff Inst. 2012. PMID: 22849236
-
Characteristics of patients with Coronavirus Disease 2019 (COVID-19) and seasonal influenza at time of hospital admission: a single center comparative study.BMC Infect Dis. 2021 Mar 17;21(1):271. doi: 10.1186/s12879-021-05957-4. BMC Infect Dis. 2021. PMID: 33731019 Free PMC article.
-
Safety and efficacy assessment of allogeneic human dental pulp stem cells to treat patients with severe COVID-19: structured summary of a study protocol for a randomized controlled trial (Phase I / II).Trials. 2020 Jun 12;21(1):520. doi: 10.1186/s13063-020-04380-5. Trials. 2020. PMID: 32532356 Free PMC article.
-
Differential diagnosis of coronavirus disease 2019 pneumonia or influenza A pneumonia by clinical characteristics and laboratory findings.J Clin Lab Anal. 2021 Feb;35(2):e23685. doi: 10.1002/jcla.23685. Epub 2021 Feb 12. J Clin Lab Anal. 2021. PMID: 33576536 Free PMC article.
-
Artificial intelligence in clinical care amidst COVID-19 pandemic: A systematic review.Comput Struct Biotechnol J. 2021;19:2833-2850. doi: 10.1016/j.csbj.2021.05.010. Epub 2021 May 7. Comput Struct Biotechnol J. 2021. PMID: 34025952 Free PMC article. Review.
Cited by
-
Use of Patient-Reported Symptom Data in Clinical Decision Rules for Predicting Influenza in a Telemedicine Setting.J Am Board Fam Med. 2023 Oct 11;36(5):766-776. doi: 10.3122/jabfm.2023.230126R1. Epub 2023 Sep 29. J Am Board Fam Med. 2023. PMID: 37775324 Free PMC article.
-
Eosinophils as potential biomarkers in respiratory viral infections.Front Immunol. 2023 Jul 6;14:1170035. doi: 10.3389/fimmu.2023.1170035. eCollection 2023. Front Immunol. 2023. PMID: 37483591 Free PMC article. Review.
-
Recent advances in understanding the role of eosinophils.Fac Rev. 2022 Sep 27;11:26. doi: 10.12703/r/11-26. eCollection 2022. Fac Rev. 2022. PMID: 36225210 Free PMC article. Review.
References
-
- World Health Organization . Situation Reports. (2020). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio... (accessed April 1, 2020).
-
- World Health Organization . WHO Director-General's Opening Remarks at the Media Briefing on COVID-19 - 11 March 2020. (2020). Available online at: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re... (accessed April 1, 2020).
-
- China Government Network . Issued by the Authority of Joint Defense and Control Mechanism of the State Council. (2020). Available online at: http://www.gov.cn/xinwen/gwylflkjz18/index.htm (accessed April 4, 2020).
LinkOut - more resources
Full Text Sources