

The Etiology of Childhood Pneumonia in Mali: Findings From the Pneumonia Etiology Research for Child Health (PERCH) Study
- PMID: 34448741
- PMCID: PMC8448406
- DOI: 10.1097/INF.0000000000002767
The Etiology of Childhood Pneumonia in Mali: Findings From the Pneumonia Etiology Research for Child Health (PERCH) Study
Abstract
Background: We present findings from the Pneumonia Etiology Research for Child Health (PERCH) site in Bamako, Mali.
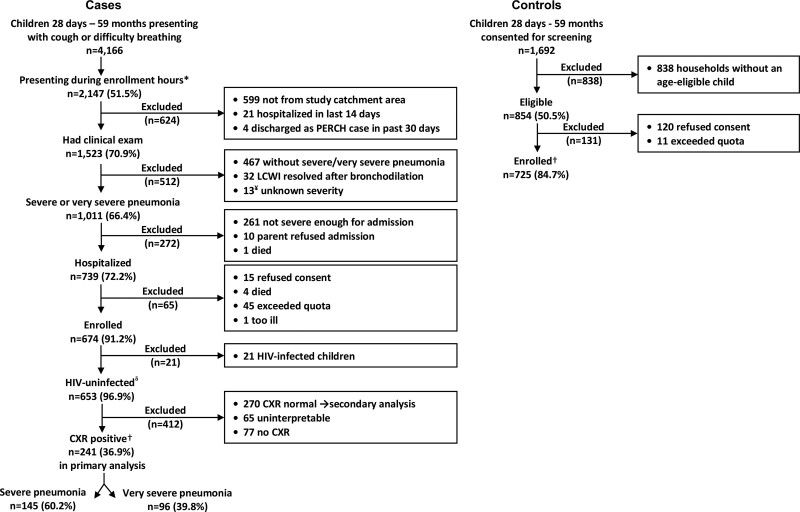
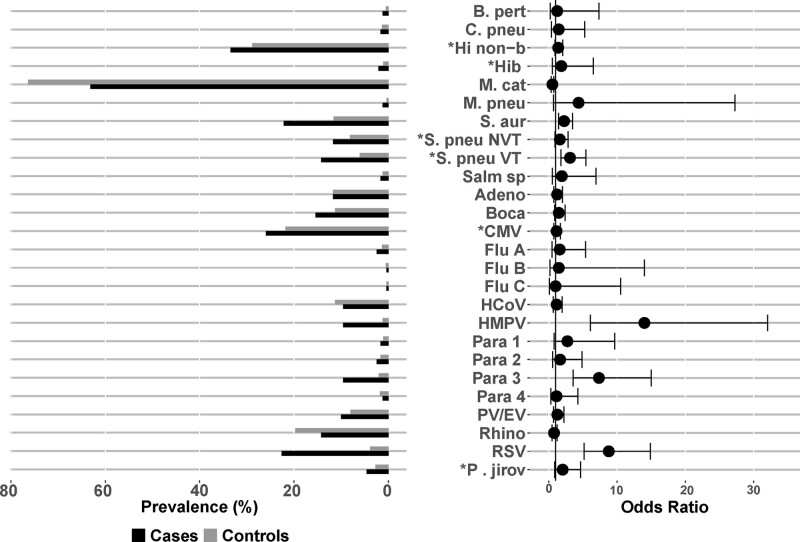
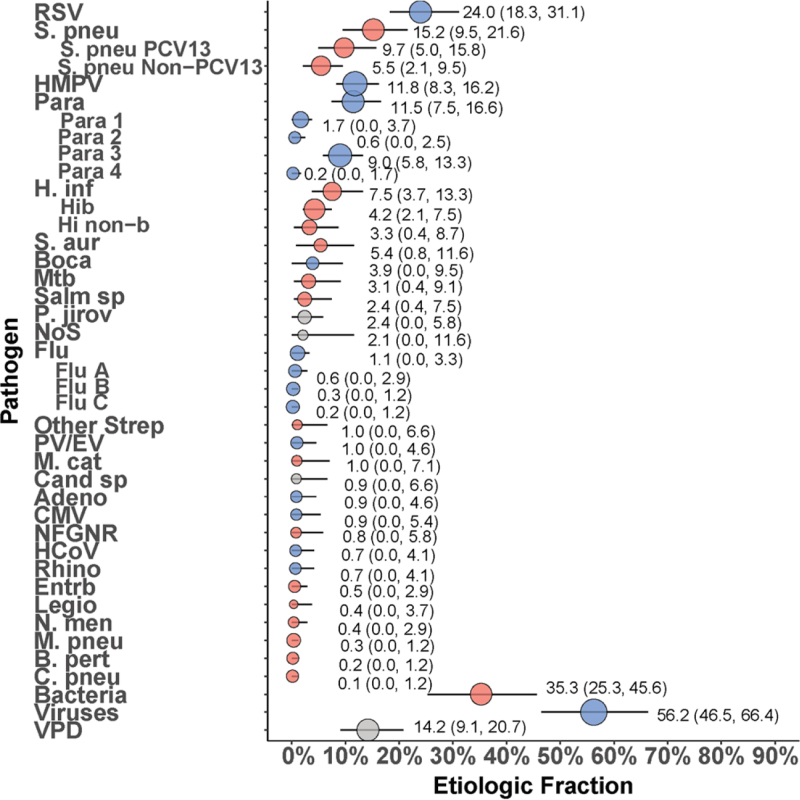
Methods: Cases were patients 28 days to 59 months of age, admitted to hospital with severe or very severe pneumonia (2005 World Health Organization definition). Community controls were frequency matched by age. Both provided nasopharyngeal and oropharyngeal swabs for multiplex polymerase chain reaction and Streptococcus pneumoniae culture. Cases underwent blood culture and induced sputum culture for Mycobacterium tuberculosis. A subset had pleural fluid and lung aspirates collected for culture and polymerase chain reaction. Primary analyses included participants with negative or unknown HIV status (HIV-) and cases with abnormal chest radiographs (CXR+). Cases and controls were compared using logistic regression adjusting for age. Etiologic fractions were calculated by a Bayesian nested partially latent class analysis, the PERCH integrated analysis.
Results: Between January 1, 2012, and January 14, 2014, we enrolled 241 CXR+/HIV- cases and 725 HIV- controls. Compared with controls, cases were more likely to have moderate-to-severe wasting (43.1% vs. 14.1%, P < 0.001) and stunting (26.6% vs. 9.4%, P < 0.001). Predominant etiologies were respiratory syncytial virus [24.0%; 95% credible interval (CrI): 18.3%-31.1%], S. pneumoniae (15.2%; 95% CrI: 9.5-21.6), human metapneumovirus (11.8%; 95% CrI: 8.3%-16.2%) and parainfluenza virus type 3 (9.0%; 95% CrI: 5.8%-13.3%). Case fatality was 13.3%, with Staphylococcus aureus, Pneumocystis jirovecii and Haemophilus influenzae type b predominating (40% of fatal cases).
Conclusions: PERCH uncovered high case fatality among children with severe pneumonia in Mali, highlighting a role for new interventions (eg, respiratory syncytial virus vaccines) and a need to improve vaccine coverage and strengthen healthcare delivery.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose. M.D.K. has received funding for consultancies from Merck, Pfizer and Novartis and grant funding from Merck. M.M.H. has received grant funding from Pfizer. L.L.H. has received grant funding from Pfizer and GlaxoSmithKline. C.P. has received grant funding from Merck. K.L.O. has received grant funding from GlaxoSmithKline and Pfizer and participated on technical advisory boards for Merck, Sanofi-Pasteur, PATH, Affinivax and ClearPath. K.L.K. has received grant funding from Merck Sharp & Dohme. The other authors have no funding or conflicts of interest to disclose.
Figures
References
-
- DHS. Mali DHS, 2012-2013 Final Report. Rockville, MD: The DHS Program, USAID; 2012–2013. Available at: https://dhsprogram.com/publications/publication-fr286-dhs-final-reports.cfm. Accessed June 20, 2019.
-
- UNICEF. Levels & Trends in Child Mortality 2017 Report. Available at: https://data.unicef.org/resources/levels-trends-child-mortality-2017/. Accessed June 20, 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
