

The Etiology of Pneumonia in HIV-uninfected Children in Kilifi, Kenya: Findings From the Pneumonia Etiology Research for Child Health (PERCH) Study
- PMID: 34448742
- PMCID: PMC8448399
- DOI: 10.1097/INF.0000000000002653
The Etiology of Pneumonia in HIV-uninfected Children in Kilifi, Kenya: Findings From the Pneumonia Etiology Research for Child Health (PERCH) Study
Abstract
Background: In the 1980s, Streptococcus pneumoniae and Haemophilus influenzae were identified as the principal causes of severe pneumonia in children. We investigated the etiology of severe childhood pneumonia in Kenya after introduction of conjugate vaccines against H. influenzae type b, in 2001, and S. pneumoniae, in 2011.
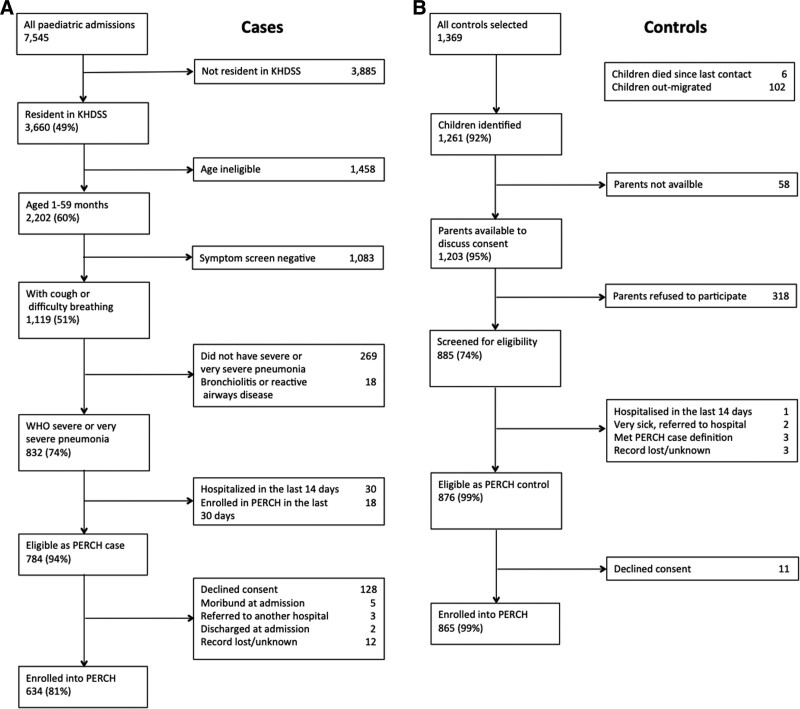
Methods: We conducted a case-control study between August 2011 and November 2013 among residents of the Kilifi Health and Demographic Surveillance System 28 days to 59 months of age. Cases were hospitalized at Kilifi County Hospital with severe or very severe pneumonia according to the 2005 World Health Organization definition. Controls were randomly selected from the community and frequency matched to cases on age and season. We tested nasal and oropharyngeal samples, sputum, pleural fluid, and blood specimens and used the Pneumonia Etiology Research for Child Health Integrated Analysis, combining latent class analysis and Bayesian methods, to attribute etiology.
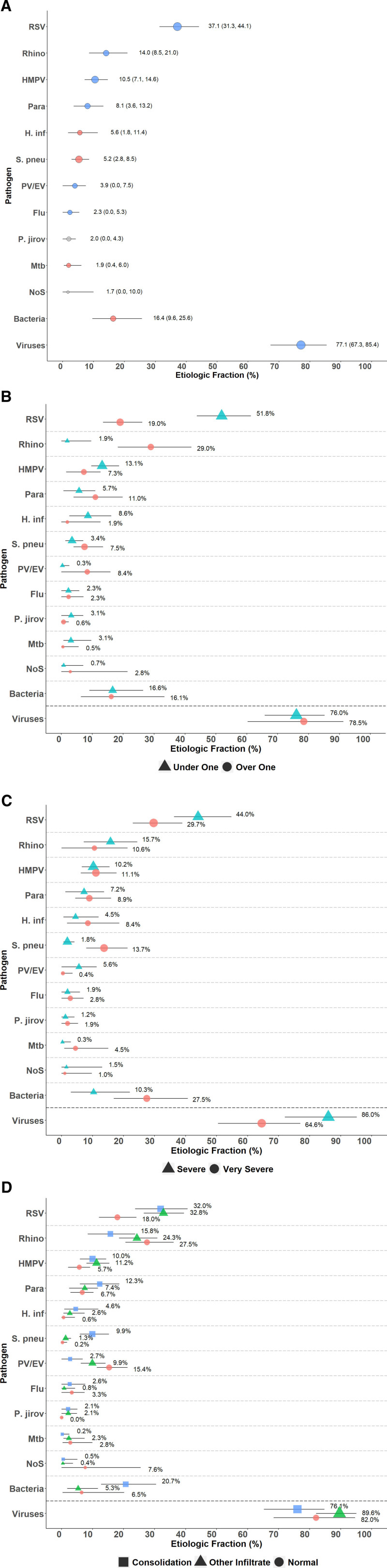
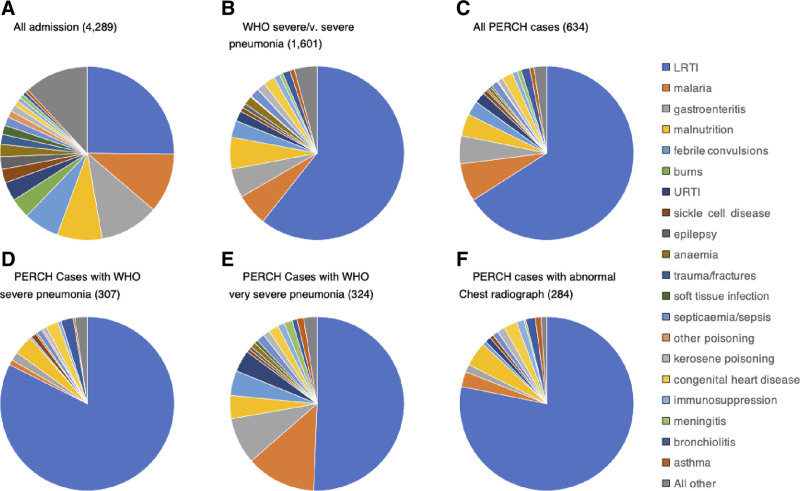
Results: We enrolled 630 and 863 HIV-uninfected cases and controls, respectively. Among the cases, 282 (44%) had abnormal chest radiographs (CXR positive), 33 (5%) died in hospital, and 177 (28%) had diagnoses other than pneumonia at discharge. Among CXR-positive pneumonia cases, viruses and bacteria accounted for 77% (95% CrI: 67%-85%) and 16% (95% CrI: 10%-26%) of pneumonia attribution, respectively. Respiratory syncytial virus, S. pneumoniae and H. influenza, accounted for 37% (95% CrI: 31%-44%), 5% (95% CrI: 3%-9%), and 6% (95% CrI: 2%-11%), respectively.
Conclusions: Respiratory syncytial virus was the main cause of CXR-positive pneumonia. The small contribution of H. influenzae type b and pneumococcus to pneumonia may reflect the impact of vaccine introductions in this population.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Liu L, Johnson HL, Cousens S, et al. ; Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151–2161. - PubMed
-
- WHO. Pocket Book of Hospital Care for Children. 2013. doi:http://dx.doi.org/10.1016/j.cardfail.2011.02.010.
-
- Hammitt LL, Crane RJ, Karani A, et al. . Effect of Haemophilus influenzae type b vaccination without a booster dose on invasive H influenzae type b disease, nasopharyngeal carriage, and population immunity in Kilifi, Kenya: a 15-year regional surveillance study. Lancet Glob Health. 2016;4:e185–e194. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
