

Adrenal myelolipomas
- PMID: 34450092
- PMCID: PMC8851410
- DOI: 10.1016/S2213-8587(21)00178-9
Adrenal myelolipomas
Abstract
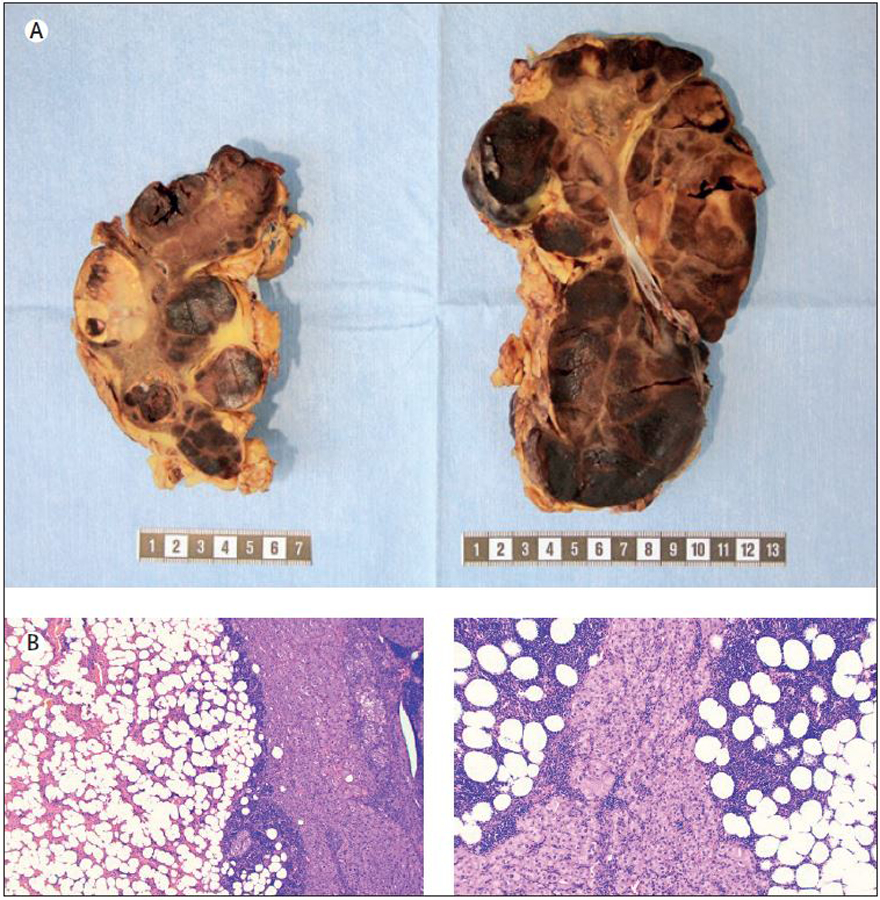
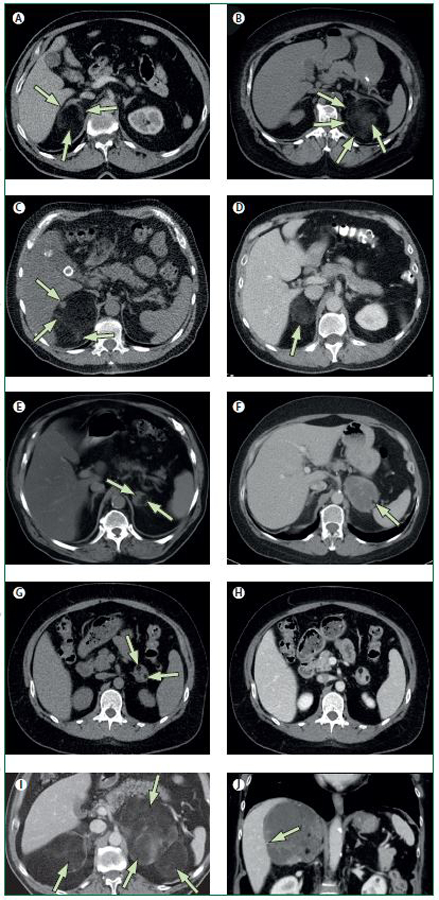
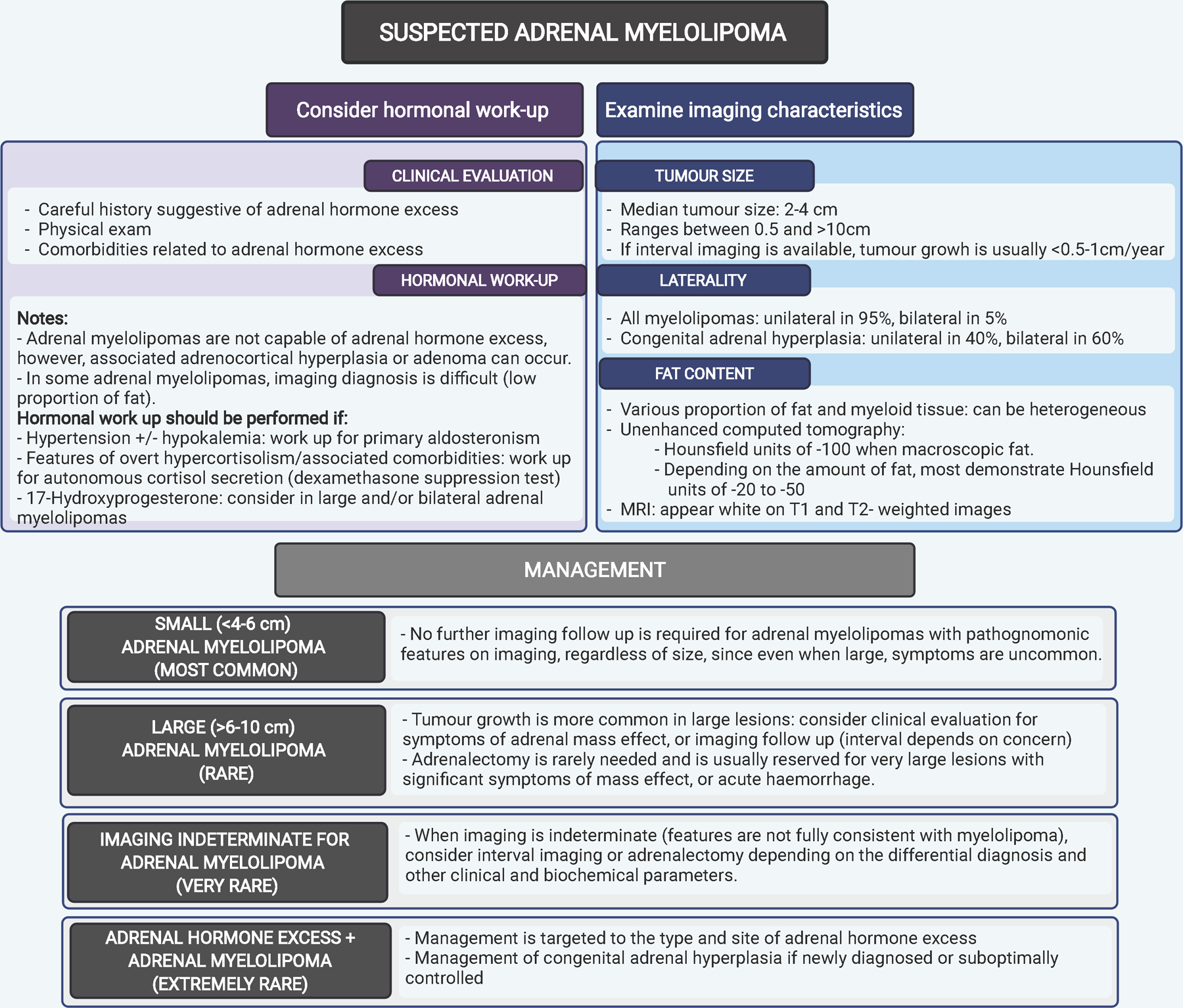
Adrenal myelolipomas are benign, lipomatous tumours with elements of myeloid cells, most of which present as adrenal incidentalomas and comprise 3·3-6·5% of all adrenal masses. Adrenal myelolipomas are usually unilateral (in 95% of cases), variable in size, most often found during midlife, and affect both sexes almost equally. On imaging, adrenal myelolipomas show pathognomonic imaging features consistent with the presence of macroscopic fat. Large adrenal myelolipomas can cause symptoms of mass effect, and can occasionally be complicated by haemorrhage. In the event of a concomitant adrenal cortical adenoma or hyperplasia, adrenal hormone excess might be detected in patients with adrenal myelolipoma. Patients with congenital adrenal hyperplasia exhibit a higher prevalence of adrenal myelolipomas than other patient groups, and are at risk of developing large and bilateral lesions. This Review discusses the pathogenesis, clinical presentation, and management of adrenal myelolipomas.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests IB is supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (NIH) USA under award K23DK121888. The views expressed are those of the authors and not necessarily those of the National Institutes of Health. IB reports consulting with Strongbridge, HRA Pharma, Corcept, CinCor, and Sparrow Pharmaceutics, and serves on the data safety board for Adrenas Therapeutics. HF has consulted for Neurocrine Biosciences, Diurnal, Roche Diagnostics International, and Adrenas Therapeutics. The other authors declare no competing interests.
Figures
References
-
- Gierke E Über Knochenmarksgewebe in der Nebenniere. Zeiglers Beitr Pathol Anat 1905; 7: 311–24.
-
- Ichijo T, Ueshiba H, Nawata H, Yanase T. A nationwide survey of adrenal incidentalomas in Japan: the first report of clinical and epidemiological features. Endocr J 2020; 67(2): 141–52. - PubMed
-
- Daneshmand S, Quek ML. Adrenal myelolipoma: diagnosis and management. Urol J 2006; 3(2): 71–4. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
