

Effect of Professional and Extra-Professional Exposure on Seroprevalence of SARS-CoV-2 Infection among Healthcare Workers of the French Alps: A Multicentric Cross-Sectional Study
- PMID: 34451949
- PMCID: PMC8402428
- DOI: 10.3390/vaccines9080824
Effect of Professional and Extra-Professional Exposure on Seroprevalence of SARS-CoV-2 Infection among Healthcare Workers of the French Alps: A Multicentric Cross-Sectional Study
Abstract
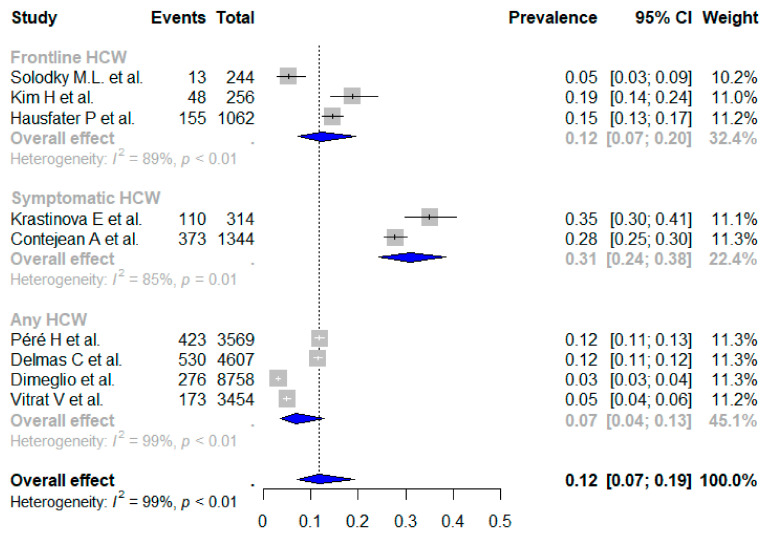
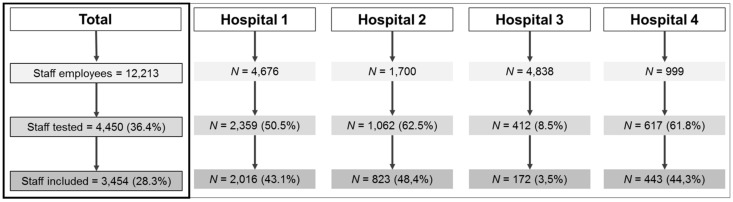
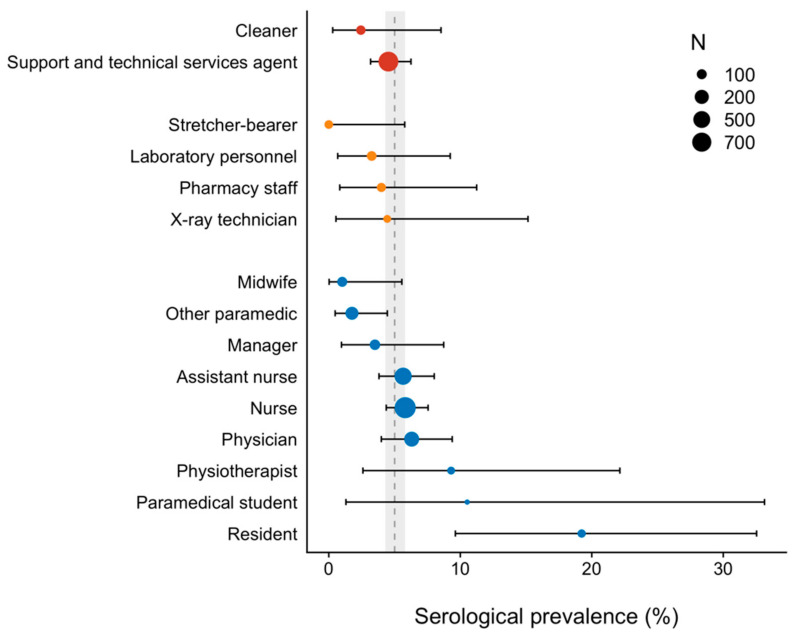
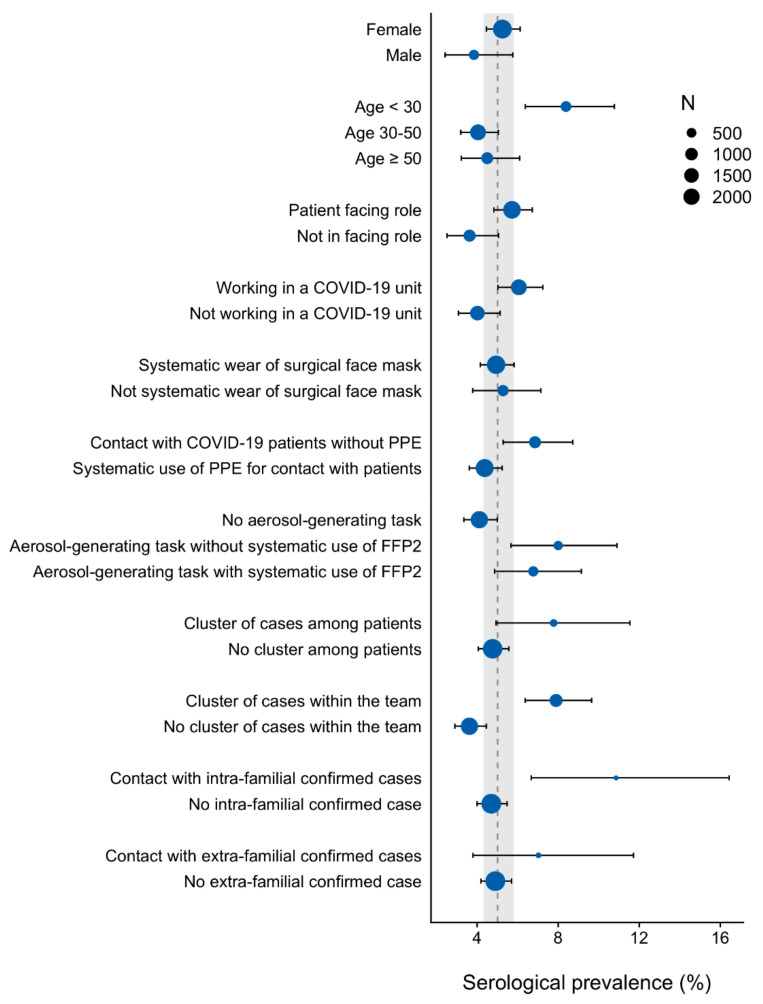
We aimed to report SARS-CoV-2 seroprevalence after the first wave of the pandemic among healthcare workers, and to explore factors associated with an increased infection rate. We conducted a multicentric cross-sectional survey from 27 June to 31 September 2020. For this survey, we enrolled 3454 voluntary healthcare workers across four participating hospitals, of which 83.4% were female, with a median age of 40.6 years old (31.8-50.3). We serologically screened the employees for SARS-CoV-2, estimated the prevalence of infection, and conducted binomial logistic regression with random effect on participating hospitals to investigate associations. We estimated the prevalence of SARS-CoV-2 infection at 5.0% (95 CI, 4.3%-5.8%). We found the lowest prevalence in health professional management support (4.3%) staff. Infections were more frequent in young professionals below 30 years old (aOR = 1.59, (95 CI, 1.06-2.37)), including paramedical students and residents (aOR = 3.38, (95 CI, 1.62-7.05)). In this group, SARS-CoV-2 prevalence was up 16.9%. The location of work and patient-facing role were not associated with increased infections. Employees reporting contacts with COVID-19 patients without adequate protective equipment had a higher rate of infection (aOR = 1.66, (95 CI, 1.12-2.44)). Aerosol-generating tasks were associated with a ~1.7-fold rate of infection, regardless of the uptake of FFP2. Those exposed to clusters of infected colleagues (aOR = 1.77, (95 CI, 1.24-2.53)) or intra-familial COVID-19 relatives (aOR = 2.09, (95 CI, 1.15-3.80)) also had a higher likelihood of infection. This report highlights that a sustained availability of personal protective equipment limits the SARS-CoV-2 infection rate to what is measured in the general population. It also pinpoints the need for dedicated hygiene training among young professionals, justifies the systematic eviction of infected personnel, and stresses the need for interventions to increase vaccination coverage among any healthcare workers.
Keywords: COVID-19; SARS-CoV-2; cross-sectional survey; healthcare workers; serologic testing.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Seroprevalence of and Risk Factors Associated With SARS-CoV-2 Infection in Health Care Workers During the Early COVID-19 Pandemic in Italy.JAMA Netw Open. 2021 Jul 1;4(7):e2115699. doi: 10.1001/jamanetworkopen.2021.15699. JAMA Netw Open. 2021. PMID: 34228126 Free PMC article.
-
Seroprevalence of SARS-CoV-2 antibodies among healthcare workers in Dutch hospitals after the 2020 first wave: a multicentre cross-sectional study with prospective follow-up.Antimicrob Resist Infect Control. 2023 Nov 29;12(1):137. doi: 10.1186/s13756-023-01324-x. Antimicrob Resist Infect Control. 2023. PMID: 38031155 Free PMC article.
-
Association between personal protective equipment and SARS-CoV-2 infection risk in emergency department healthcare workers.Eur J Emerg Med. 2021 Jun 1;28(3):202-209. doi: 10.1097/MEJ.0000000000000766. Eur J Emerg Med. 2021. PMID: 33105329 Free PMC article.
-
Seroprevalence of SARS-CoV-2 antibodies and associated factors in healthcare workers: a systematic review and meta-analysis.J Hosp Infect. 2021 Feb;108:120-134. doi: 10.1016/j.jhin.2020.11.008. Epub 2020 Nov 16. J Hosp Infect. 2021. PMID: 33212126 Free PMC article.
-
Prevalence of SARS-CoV-2 antibodies among nurses: A systematic review and meta-analysis.J Clin Nurs. 2022 Jun;31(11-12):1557-1569. doi: 10.1111/jocn.16009. Epub 2021 Sep 27. J Clin Nurs. 2022. PMID: 34570947 Free PMC article.
Cited by
-
Risk of transmission of respiratory viruses during aerosol-generating medical procedures (AGMPs) revisited in the COVID-19 pandemic: a systematic review.Antimicrob Resist Infect Control. 2022 Aug 11;11(1):102. doi: 10.1186/s13756-022-01133-8. Antimicrob Resist Infect Control. 2022. PMID: 35953854 Free PMC article.
-
Risk and protective factors for severe acute respiratory coronavirus virus 2 (SARS-CoV-2) infection among healthcare workers: A test-negative case-control study in Québec, Canada.Infect Control Hosp Epidemiol. 2023 Jul;44(7):1121-1130. doi: 10.1017/ice.2022.231. Epub 2022 Sep 9. Infect Control Hosp Epidemiol. 2023. PMID: 36082690 Free PMC article.
-
SARS-CoV-2 infection among healthcare workers: the role of occupational and household exposures during the first three pandemic waves in Quebec, Canada.Antimicrob Steward Healthc Epidemiol. 2023 Oct 20;3(1):e180. doi: 10.1017/ash.2023.442. eCollection 2023. Antimicrob Steward Healthc Epidemiol. 2023. PMID: 38028905 Free PMC article.
-
Outbreaks of COVID-19 in Nursing Homes: A Cross-Sectional Survey of 74 Nursing Homes in a French Area.J Clin Med. 2021 Sep 21;10(18):4280. doi: 10.3390/jcm10184280. J Clin Med. 2021. PMID: 34575392 Free PMC article.
-
Effectiveness of inactivated COVID-19 vaccines against SARS-CoV-2 infections among healthcare personnel in Pakistan: a test-negative case-control study.BMJ Open. 2023 Jun 27;13(6):e071789. doi: 10.1136/bmjopen-2023-071789. BMJ Open. 2023. PMID: 37369396 Free PMC article.
References
-
- Shah A.S.V., Wood R., Gribben C., Caldwell D., Bishop J., Weir A., Kennedy S., Reid M., Smith-Palmer A., Goldberg D., et al. Risk of hospital admission with coronavirus disease 2019 in healthcare workers and their households: Nationwide linkage cohort study. BMJ. 2020;371:m3582. doi: 10.1136/bmj.m3582. - DOI - PMC - PubMed
-
- Martin C., Montesinos I., Dauby N., Gilles C., Dahma H., Van Den Wijngaert S., De Wit S., Delforge M., Clumeck N., Vandenberg O. Dynamics of SARS-CoV-2 RT-PCR positivity and seroprevalence among high-risk healthcare workers and hospital staff. J. Hosp. Infect. 2020;106:102–106. doi: 10.1016/j.jhin.2020.06.028. - DOI - PMC - PubMed
-
- Solodky M.L., Galvez C., Russias B., Detourbet P., N’Guyen-Bonin V., Herr A.-L., Zrounba P., Blay J.-Y. Lower detection rates of SARS-COV2 antibodies in cancer patients versus health care workers after symptomatic COVID-19. Ann. Oncol. 2020;31:1087–1088. doi: 10.1016/j.annonc.2020.04.475. - DOI - PMC - PubMed
-
- Guery R., Delaye C., Brule N., Nael V., Castain L., Raffi F., De Decker L. Limited effectiveness of systematic screening by nasopharyngeal RT-PCR of medicalized nursing home staff after a first case of COVID-19 in a resident. Med. Mal. Infect. 2020;50:748–750. doi: 10.1016/j.medmal.2020.04.020. - DOI - PMC - PubMed
-
- Contejean A., Leporrier J., Canouï E., Alby-Laurent F., Lafont E., Beaudeau L., Parize P., Lecieux F., Greffet A., Chéron G., et al. Comparing dynamics and determinants of SARS-CoV-2 transmissions among health care workers of adult and pediatric settings in central Paris. Clin. Infect. Dis. 2020 doi: 10.1093/cid/ciaa977. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
