

The impact of Healthy Conversation Skills training on health professionals' barriers to having behaviour change conversations: a pre-post survey using the Theoretical Domains Framework
- PMID: 34452634
- PMCID: PMC8394191
- DOI: 10.1186/s12913-021-06893-4
The impact of Healthy Conversation Skills training on health professionals' barriers to having behaviour change conversations: a pre-post survey using the Theoretical Domains Framework
Abstract
Background: Changing people's behaviour by giving advice and instruction, as traditionally provided in healthcare consultations, is usually ineffective. Healthy Conversation Skills (HCS) training enhances health professionals' communication skills and ability to empower and motivate people in health behaviour change. Guided by the Theoretical Domains Framework (TDF), this study examined the impact of HCS training on health professional barriers to conducting behaviour change conversations in both clinical and non-clinical settings. Secondary aims were to i) identify health professionals' barriers to having behaviour change conversations, and explore the ii) effect of HCS training on health professionals' competence and attitudes to adopting HCS, iii) feasibility, acceptability and appropriateness of using HCS in their clinical and non-clinical roles, and iv) acceptability and quality of HCS training.
Methods: HCS training was conducted in October-November 2019 and February 2020. Pre-training (T1), post-training (T2) and follow-up (T3; 6-10 weeks post-training) surveys collected data on demographics and changes in competence, confidence, importance and usefulness (10-point Likert scale, where 10 = highest score) of conducting behaviour change conversations. Validated items assessing barriers to having these conversations were based on eight TDF domains. Post-training acceptability and quality of training was assessed. Data were summarised using descriptive statistics, and differences between TDF domain scores at the specific time points were analysed using Wilcoxon matched-pairs signed-rank tests.
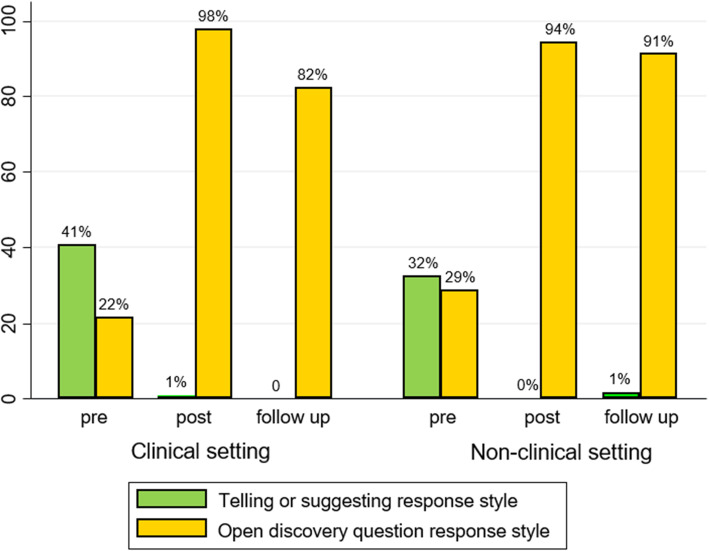
Results: Sixty-four participants consented to complete surveys (97% women; 16% identified as Aboriginal), with 37 employed in clinical settings and 27 in non-clinical settings. The training improved scores for the TDF domains of skills (T1: median (interquartile range) = 4.7(3.3-5.3); T3 = 5.7(5.3-6.0), p < 0.01), belief about capabilities (T1 = 4.7(3.3-6.0); T3 = 5.7(5.0-6.0), p < 0.01), and goals (T1 = 4.3(3.7-5.0); T3 = 4.7(4.3-5.3), p < 0.01) at follow-up. Competence in using 'open discovery questions' increased post-training (T1 = 25% of responses; T2 = 96% of responses; T3 = 87% of responses, p < 0.001), as did participants' confidence for having behaviour change conversations (T1 = 6.0(4.7-7.6); T2 = 8.1(7.1-8.8), p < 0.001), including an increased confidence in having behaviour change conversations with Aboriginal clients (T1 = 5.0(2.7-6.3); T2 = 7.6(6.4-8.3), p < 0.001).
Conclusions: Provision of additional support strategies to address intentions; memory, attention and decision processes; and behavioural regulation may enhance adoption and maintenance of HCS in routine practice. Wider implementation of HCS training could be an effective strategy to building capacity and support health professionals to use a person-centred, opportunistic approach to health behaviour change.
Keywords: Behaviour change theory; Communication skills; Health promotion; Healthy Conversation Skills; Theoretical Domains Framework; Workforce development.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Evaluating a train-the-trainer model for scaling-up Healthy Conversation Skills training: A pre-post survey using the Theoretical Domains Framework.Patient Educ Couns. 2022 Oct;105(10):3078-3085. doi: 10.1016/j.pec.2022.06.011. Epub 2022 Jun 21. Patient Educ Couns. 2022. PMID: 35779983 Review.
-
Delivering an iterative Communication Partner Training programme to multidisciplinary healthcare professionals: A pilot implementation study and process evaluation.Int J Lang Commun Disord. 2021 May;56(3):620-636. doi: 10.1111/1460-6984.12618. Epub 2021 Apr 5. Int J Lang Commun Disord. 2021. PMID: 33818902
-
Increasing confidence and competence in supporting behaviour change in physiotherapy practice using Making Every Contact Count Healthy Conversation Skills: a before and after evaluation.BMC Health Serv Res. 2025 Jun 4;25(1):797. doi: 10.1186/s12913-025-12513-2. BMC Health Serv Res. 2025. PMID: 40468316 Free PMC article.
-
'It's difficult, I think it's complicated': Health care professionals' barriers and enablers to providing opportunistic behaviour change interventions during routine medical consultations.Br J Health Psychol. 2019 Sep;24(3):571-592. doi: 10.1111/bjhp.12368. Epub 2019 Apr 12. Br J Health Psychol. 2019. PMID: 30977291 Free PMC article.
-
Use of the behaviour change wheel to improve everyday person-centred conversations on physical activity across healthcare.BMC Public Health. 2022 Sep 20;22(1):1784. doi: 10.1186/s12889-022-14178-6. BMC Public Health. 2022. PMID: 36127688 Free PMC article. Review.
Cited by
-
How useful is the Making Every Contact Count Healthy Conversation Skills approach for supporting people with musculoskeletal conditions?Z Gesundh Wiss. 2022;30(10):2389-2405. doi: 10.1007/s10389-022-01718-y. Epub 2022 May 4. Z Gesundh Wiss. 2022. PMID: 35530417 Free PMC article.
-
The effectiveness of medical nutrition therapy for people at moderate to high risk of cardiovascular disease in an Australian rural primary care setting: 12-month results from a pragmatic cluster randomised controlled trial.BMC Health Serv Res. 2025 Jul 16;25(1):956. doi: 10.1186/s12913-025-13096-8. BMC Health Serv Res. 2025. PMID: 40671037 Free PMC article. Clinical Trial.
-
Developing a telehealth medical nutrition therapy (MNT) service for adults living in rural Australia at risk of cardiovascular disease: An intervention development study.J Hum Nutr Diet. 2023 Oct;36(5):1782-1794. doi: 10.1111/jhn.13193. Epub 2023 Jun 21. J Hum Nutr Diet. 2023. PMID: 37344944 Free PMC article. Clinical Trial.
-
Multimorbidity in Difficult Asthma: The Need for Personalised and Non-Pharmacological Approaches to Address a Difficult Breathing Syndrome.J Pers Med. 2022 Aug 31;12(9):1435. doi: 10.3390/jpm12091435. J Pers Med. 2022. PMID: 36143220 Free PMC article. Review.
-
A single-blind, parallel-group randomised trial of a Technology-assisted and remotely delivered Cognitive Behavioural Therapy intervention (Tech-CBT) versus usual care to reduce anxiety in people with mild cognitive impairment and dementia: study protocol for a randomised trial.Trials. 2023 Jun 20;24(1):420. doi: 10.1186/s13063-023-07381-2. Trials. 2023. PMID: 37340492 Free PMC article.
References
-
- World Health Organization . Noncommunicable diseases progress monitor 2020. Geneva: World Health Organization; 2020.
-
- Marteau TM, Hollands GJ, Kelly MP. Emerging behavioral and social science perspectives on population health. Bethesda, MD: National Institutes of Health/Agency For Healthcare Research and Quality; 2015. Changing population behavior and reducing health disparities: exploring the potential of “choice architecture” interventions; pp. 105–126.
MeSH terms
LinkOut - more resources
Full Text Sources
