

Indirect effects of COVID-19 on maternal, neonatal, child, sexual and reproductive health services in Kampala, Uganda
- PMID: 34452941
- PMCID: PMC8406460
- DOI: 10.1136/bmjgh-2021-006102
Indirect effects of COVID-19 on maternal, neonatal, child, sexual and reproductive health services in Kampala, Uganda
Abstract
Background: COVID-19 impacted global maternal, neonatal and child health outcomes. We hypothesised that the early, strict lockdown that restricted individuals' movements in Uganda limited access to services.
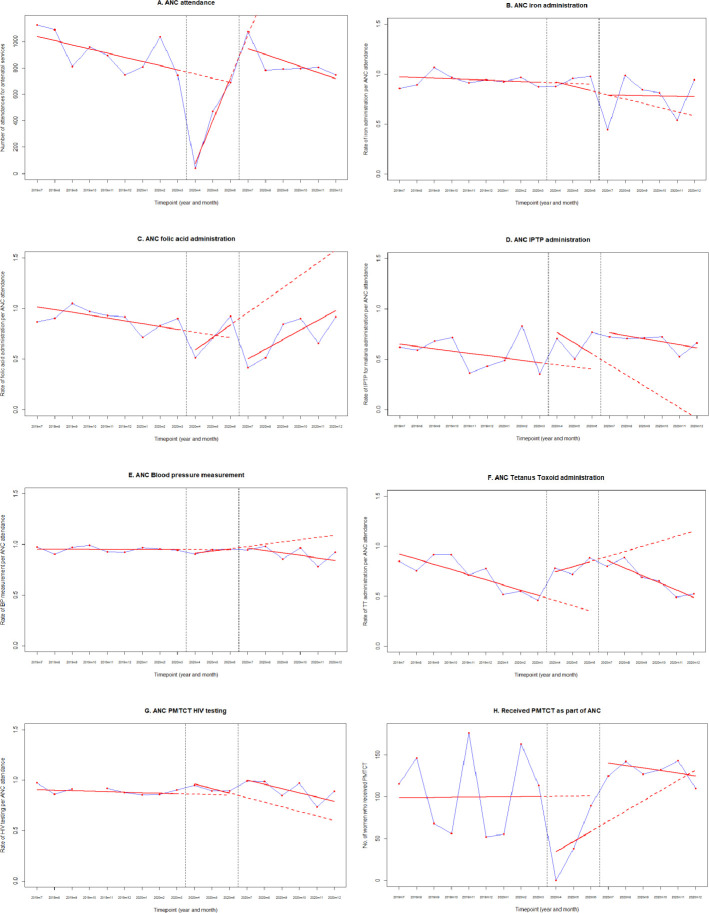
Methods: An observational study, using routinely collected data from Electronic Medical Records, was carried out, in Kawempe district, Kampala. An interrupted time series analysis assessed the impact on maternal, neonatal, child, sexual and reproductive health services from July 2019 to December 2020. Descriptive statistics summarised the main outcomes before (July 2019-March 2020), during (April 2020-June 2020) and after the national lockdown (July 2020-December 2020).
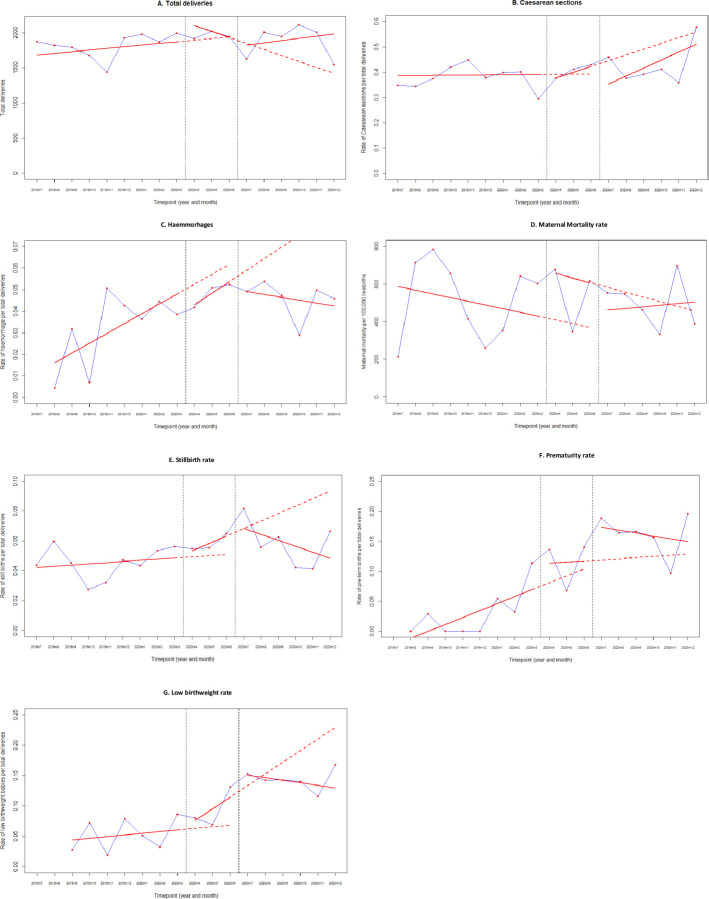
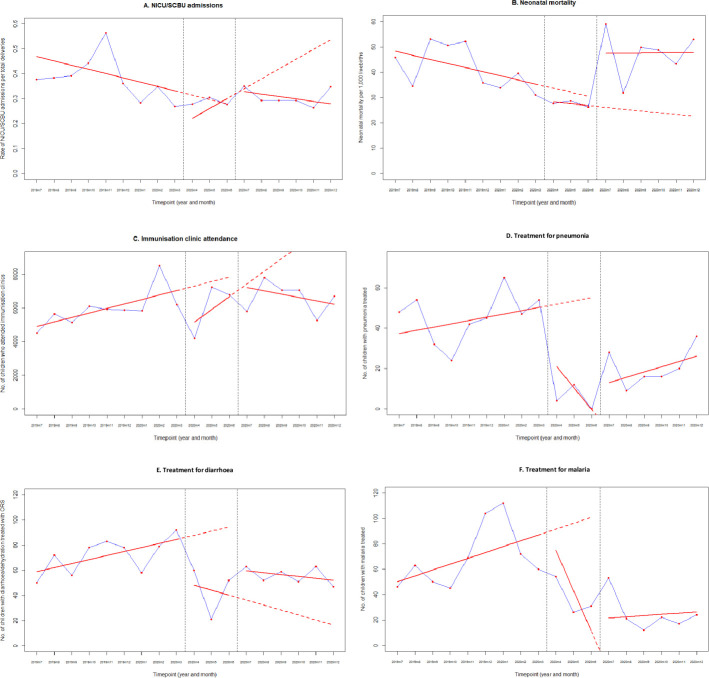
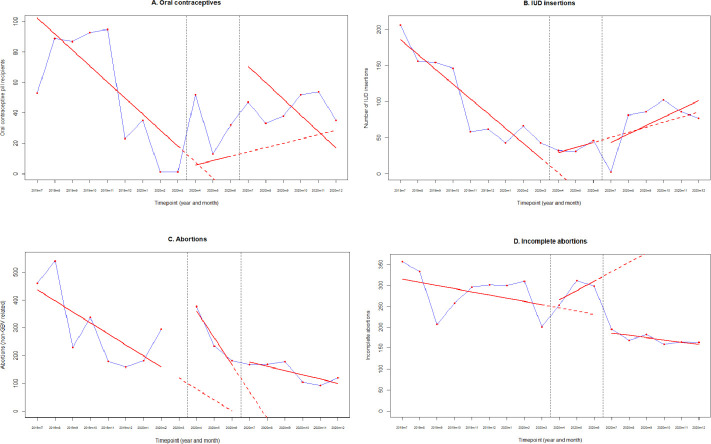
Results: Between 1 July 2019 and 31 December 2020, there were 14 401 antenatal clinic, 33 499 deliveries, 111 658 childhood service and 57 174 sexual health attendances. All antenatal and vaccination services ceased in lockdown for 4 weeks.During the 3-month lockdown, the number of antenatal attendances significantly decreased and remain below pre-COVID levels (370 fewer/month). Attendances for prevention of mother-to-child transmission of HIV dropped then stabilised. Increases during lockdown and immediately postlockdown included the number of women treated for high blood pressure, eclampsia and pre-eclampsia (218 more/month), adverse pregnancy outcomes (stillbirths, low-birth-weight and premature infant births), the rate of neonatal unit admissions, neonatal deaths and abortions. Maternal mortality remained stable. Immunisation clinic attendance declined while neonatal death rate rose (from 39 to 49/1000 livebirths). The number of children treated for pneumonia, diarrhoea and malaria decreased during lockdown.
Conclusion: The Ugandan response to COVID-19 negatively impacted maternal, child and neonatal health, with an increase seen in pregnancy complications and fetal and infant outcomes, likely due to delayed care-seeking behaviour. Decreased vaccination clinic attendance leaves a cohort of infants unprotected, affecting all vaccine-preventable diseases. Future pandemic responses must consider impacts of movement restrictions and access to preventative services to protect maternal and child health.
Keywords: COVID-19; child health; maternal health; public health; vaccines.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- COVID-19 response in the world Health organization African region 2020.
-
- World Health Organization . The coronavirus disease 2019 (COVID-19) strategic preparedness and response plan for the WHO Africa region: 1 February 2021 - 31 January 2022. World Health Organization, 2021.
-
- Uganda: Johns Hopkins University & Medicine, 2021. Available: https://coronavirus.jhu.edu/region/uganda [Accessed 06 Jul 2021].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous