

The PEMDAC phase 2 study of pembrolizumab and entinostat in patients with metastatic uveal melanoma
- PMID: 34453044
- PMCID: PMC8397717
- DOI: 10.1038/s41467-021-25332-w
The PEMDAC phase 2 study of pembrolizumab and entinostat in patients with metastatic uveal melanoma
Abstract
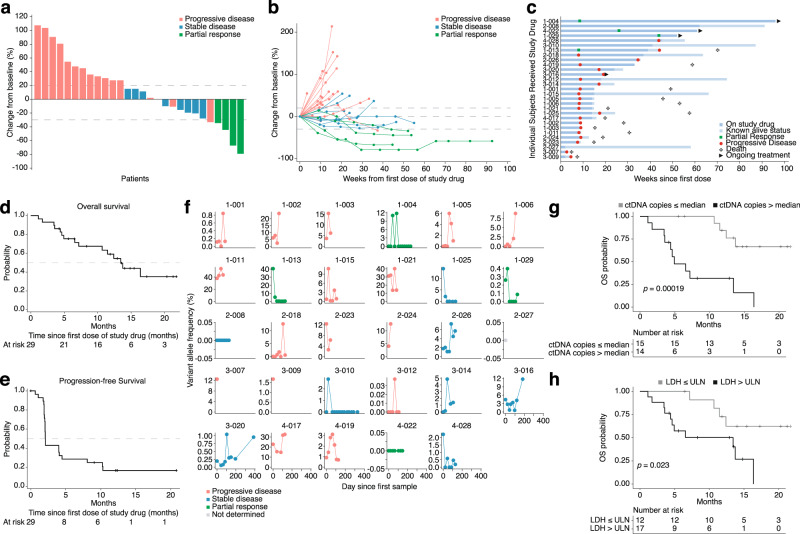
Preclinical studies have suggested that epigenetic therapy could enhance immunogenicity of cancer cells. We report the results of the PEMDAC phase 2 clinical trial (n = 29; NCT02697630) where the HDAC inhibitor entinostat was combined with the PD-1 inhibitor pembrolizumab in patients with metastatic uveal melanoma (UM). The primary endpoint was objective response rate (ORR), and was met with an ORR of 14%. The clinical benefit rate at 18 weeks was 28%, median progression free survival was 2.1 months and the median overall survival was 13.4 months. Toxicities were manageable, and there were no treatment-related deaths. Objective responses and/or prolonged survival were seen in patients with BAP1 wildtype tumors, and in one patient with an iris melanoma that exhibited a UV signature. Longer survival also correlated with low baseline ctDNA levels or LDH. In conclusion, HDAC inhibition and anti-PD1 immunotherapy results in durable responses in a subset of patients with metastatic UM.Trial registration ClinicalTrials.gov registration number: NCT02697630 (registered 3 March 2016). EudraCT registration number: 2016-002114-50.
© 2021. The Author(s).
Conflict of interest statement
Lars Ny received a research grant from MSD and Syndax Pharmaceuticals to support some aspects of the PEMDAC study. Anders Ståhlberg is the coinventor of SiMSen-Seq (ctDNA measurement), is a board member of, and has stock ownership in SiMSen Diagnostics. The remaining authors declare no conflict of interest.
Figures


References
-
- Bergman L, et al. Incidence of uveal melanoma in Sweden from 1960 to 1998. Invest. Ophthalmol. Vis. Sci. 2002;43:2579–2583. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
