

Clinical outcomes of frozen autograft reconstruction for the treatment of primary bone sarcoma in adolescents and young adults
- PMID: 34453061
- PMCID: PMC8397769
- DOI: 10.1038/s41598-021-96162-5
Clinical outcomes of frozen autograft reconstruction for the treatment of primary bone sarcoma in adolescents and young adults
Abstract
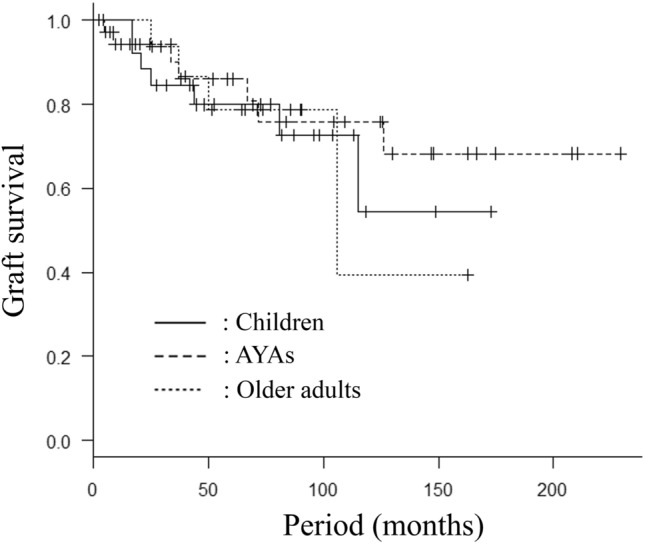
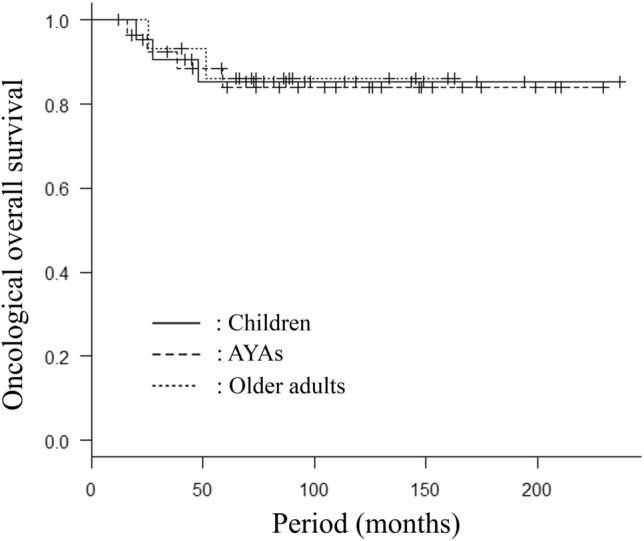
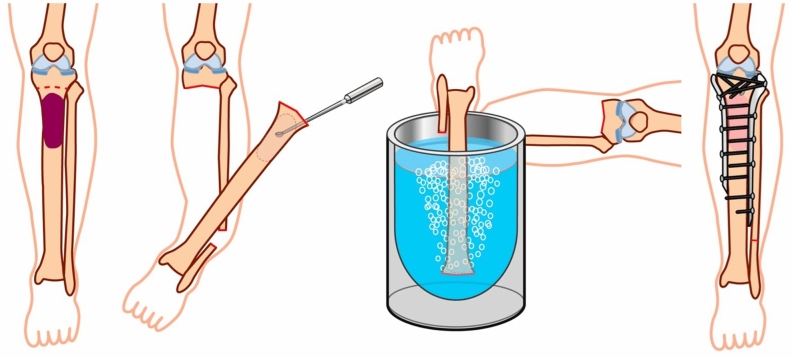
Age affects the clinical outcomes of cancer treatment, including those for bone sarcoma. Successful reconstruction using frozen autograft after excision of bone sarcoma has been reported; however, little is known about the clinical outcomes of frozen autograft reconstruction according to age. The purpose was to evaluate the clinical outcomes of the frozen autograft reconstruction focusing on skeletally mature adolescents and young adults (AYAs) that was 15 to 39 years of age. A total of 37 AYA patients with primary bone sarcoma on the appendicular skeleton were enrolled in this study. The mean follow-up period was 89 months. The graft survival (GS), overall survival (OS), recurrence-free survival (RFS), complications and the function were retrospectively evaluated using medical records. The 10-year GS, OS, and RFS rates were 76%, 84%, and 79%, respectively. Bone union was achieved with a rate of 94% within 1 year after surgery, and nonunion (n = 1) and fracture (n = 2) were infrequently observed. Graft removal was performed in 7 cases, and the most common reason for the removal was infection (n = 5). The Musculoskeletal Tumor Society score was excellent in 23 cases of the available 29 cases. Frozen autograft reconstruction for AYAs showed excellent clinical outcomes, although the long-term follow-up is required.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Fletcher CD, et al. WHO Classification of Tumours. Soft Tissue and Bone Tumours. 4. IARC; 2013.
-
- Closing the Gap: Research and care imperatives for adolescents and young adults with cancer. Report of the Adolescent and Young Adult Oncology Progress Review Group. (2006).
-
- Kim CY, Collier CD, Liu RW, Getty PJ. Are limb-sparing surgical resections comparable to amputation for patients with pelvic chondrosarcoma? A case-control, propensity score-matched analysis of the national cancer database. Clin. Orthop. Relat. Res. 2019;477(3):596–605. doi: 10.1097/CORR.0000000000000622. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
