

Non-traditional implantable cardioverter-defibrillator configurations and insertion techniques: a review of contemporary options
- PMID: 34453529
- PMCID: PMC8824518
- DOI: 10.1093/europace/euab178
Non-traditional implantable cardioverter-defibrillator configurations and insertion techniques: a review of contemporary options
Abstract
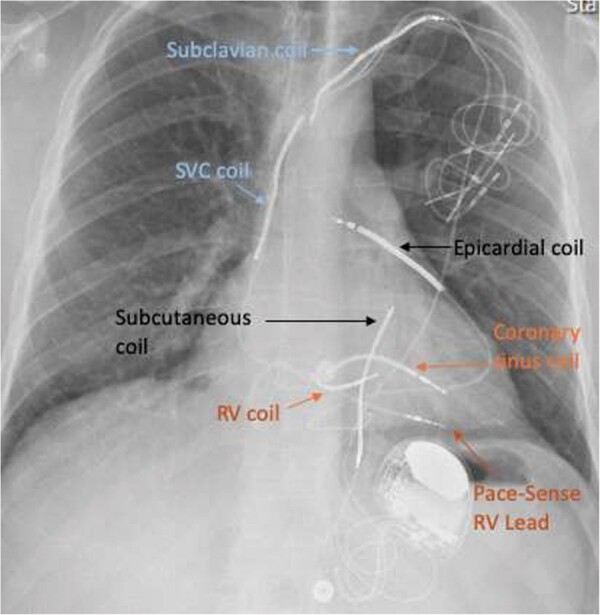
Implantable cardioverter-defibrillators (ICDs) have revolutionized the treatment of acquired or inherited cardiac diseases associated with a high risk of sudden cardiac death due to ventricular tachyarrhythmias. Contemporary ICD devices offer reliable arrhythmia detection and discrimination algorithms and deliver highly efficient tachytherapies. Percutaneously inserted transvenous defibrillator coils with pectoral generator placement are the first-line approach in the majority of adults due to their extensively documented clinical benefit and efficiency with comparably low periprocedural implantation risks as well as the option of providing pain-free tachycardia treatment via anti-tachycardia pacing (ATP), concomitant bradycardiaprotection, and incorporation in a cardiac resynchronization therapy if indicated. Yet, expanding ICD indications particularly among younger and more complex patient groups as well as the increasingly evident long-term consequences and complications associated with intravascular lead placements promoted the development of alternative ICD configurations. Most established in daily clinical practice is the subcutaneous ICD but other innovative extravascular approaches like epicardial, pericardial, extra-pleural, and most recently substernal defibrillator coil placements have been introduced as well to overcome shortcomings associated with traditional devices and allow for individualized treatment strategies tailored to the patients characteristics and needs. The review aims to provide practical solutions for common complications encountered with transvenous ICD systems including restricted venous access, high defibrillation/fibrillation thresholds (DFTs), and recurrent device infections. We summarize the contemporary options for non-traditional extravascular ICD configurations outlining indications, advantages, and disadvantages.
Keywords: Epicardial implantable cardioverter-defibrillator; Extra-pleural implantable cardioverter-defibrillator; High defibrillation/fibrillation threshold; Hybrid implantable cardioverter-defibrillator configurations; Non-traditional implantable cardioverter-defibrillator; Subcutaneous implantable cardioverter-defibrillator; Substernal implantable cardioverter-defibrillator; Venous access crisis.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Boczar K, Ząbek A, Haberka K, Hardzina M, Dębski M, Rydlewska A et al. Venous stenosis and occlusion in the presence of endocardial leads. Adv Clin Exp Med 2016;25:83–91. - PubMed
-
- Hauser RG, Hayes DL. Increasing hazard of Sprint Fidelis implantable cardioverter-defibrillator lead failure. Heart Rhythm 2009;6:605–10. - PubMed
-
- Hsu JC, Varosy PD, Bao H, Dewland TA, Curtis JP, Marcus GM. Cardiac perforation from implantable cardioverter defibrillator lead placement. Insights from the National. Circ Cardiovasc Qual Outcomes 2013;6:582–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
