

Clinical Cholera Surveillance Sensitivity in Bangladesh and Implications for Large-Scale Disease Control
- PMID: 34453539
- PMCID: PMC8687068
- DOI: 10.1093/infdis/jiab418
Clinical Cholera Surveillance Sensitivity in Bangladesh and Implications for Large-Scale Disease Control
Abstract
Background: A surveillance system that is sensitive to detecting high burden areas is critical for achieving widespread disease control. In 2014, Bangladesh established a nationwide, facility-based cholera surveillance system for Vibrio cholerae infection. We sought to measure the sensitivity of this surveillance system to detect cases to assess whether cholera elimination targets outlined by the Bangladesh national control plan can be adequately measured.
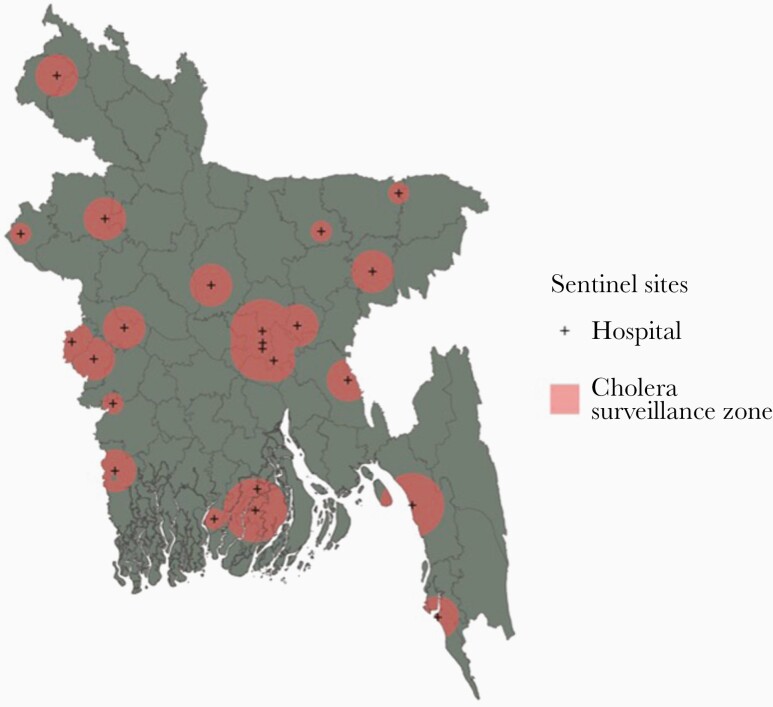
Methods: We overlaid maps of nationally representative annual V cholerae seroincidence onto maps of the catchment areas of facilities where confirmatory laboratory testing for cholera was conducted, and we identified its spatial complement as surveillance greyspots, areas where cases likely occur but go undetected. We assessed surveillance system sensitivity and changes to sensitivity given alternate surveillance site selection strategies.
Results: We estimated that 69% of Bangladeshis (111.7 million individuals) live in surveillance greyspots and that 23% (25.5 million) of these individuals live in areas with the highest V cholerae infection rates.
Conclusions: The cholera surveillance system in Bangladesh has the ability to monitor progress towards cholera elimination goals among 31% of the country's population, which may be insufficient for accurately measuring progress. Increasing surveillance coverage, particularly in the highest risk areas, should be considered.
Keywords: Bangladesh; cholera; disease control; elimination; surveillance.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures


Similar articles
-
Vibrio cholerae O1 transmission in Bangladesh: insights from a nationally representative serosurvey.Lancet Microbe. 2020 Dec;1(8):e336-e343. doi: 10.1016/S2666-5247(20)30141-5. Lancet Microbe. 2020. PMID: 33345203 Free PMC article.
-
Acute Watery Diarrhea Surveillance During the Rohingya Crisis 2017-2019 in Cox's Bazar, Bangladesh.J Infect Dis. 2021 Dec 20;224(12 Suppl 2):S717-S724. doi: 10.1093/infdis/jiab453. J Infect Dis. 2021. PMID: 34528689 Free PMC article.
-
Incidence of severe diarrhoea due to Vibrio cholerae in the catchment area of six surveillance hospitals in Bangladesh.Epidemiol Infect. 2016 Apr;144(5):927-39. doi: 10.1017/S0950268815002174. Epub 2015 Sep 22. Epidemiol Infect. 2016. PMID: 26391481 Free PMC article.
-
[Laboratory diagnosis of cholera: analysis and prospects for improvement].Klin Lab Diagn. 2009 Nov;(11):51-5. Klin Lab Diagn. 2009. PMID: 20030273 Review. Russian.
-
Emergence of a new cholera pandemic: molecular analysis of virulence determinants in Vibrio cholerae O139 and development of a live vaccine prototype.J Infect Dis. 1994 Aug;170(2):278-83. doi: 10.1093/infdis/170.2.278. J Infect Dis. 1994. PMID: 8035010 Review.
Cited by
-
National Hospital-Based Sentinel Surveillance for Cholera in Bangladesh: Epidemiological Results from 2014 to 2021.Am J Trop Med Hyg. 2023 Aug 14;109(3):575-583. doi: 10.4269/ajtmh.23-0074. Print 2023 Sep 6. Am J Trop Med Hyg. 2023. PMID: 37580033 Free PMC article.
-
Expanding cholera serosurveillance to vaccinated populations.medRxiv [Preprint]. 2025 Mar 11:2025.03.09.25323598. doi: 10.1101/2025.03.09.25323598. medRxiv. 2025. PMID: 40162250 Free PMC article. Preprint.
-
Identifying Recent Cholera Infections Using a Multiplex Bead Serological Assay.mBio. 2022 Dec 20;13(6):e0190022. doi: 10.1128/mbio.01900-22. Epub 2022 Oct 26. mBio. 2022. PMID: 36286520 Free PMC article.
-
Water pollution, cholera, and the role of probiotics: a comprehensive review in relation to public health in Bangladesh.Front Microbiol. 2025 Jan 14;15:1523397. doi: 10.3389/fmicb.2024.1523397. eCollection 2024. Front Microbiol. 2025. PMID: 39877756 Free PMC article. Review.
References
-
- Khan AI, Rashid MM, Islam MT, et al. Epidemiology of cholera in Bangladesh: findings from nationwide hospital-based surveillance, 2014-2018. Clin Infect Dis 2020; 71:1635–i42. - PubMed
-
- DGHS, MOHFW, Government of Bangladesh. Practical approach to controlling cholera in Bangladesh through dual interventions of OCV & WaSH. Available at: https://www.gtfcc.org/wp-content/uploads/2020/08/6th-annual-meeting-gtfc.... Accessed 10 May 2021.
-
- Centers for Disease Control (CDC). Guidelines for evaluating surveillance systems. MMWR Suppl 1988; 37:1–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
