

Cellular immunity predominates over humoral immunity after homologous and heterologous mRNA and vector-based COVID-19 vaccine regimens in solid organ transplant recipients
- PMID: 34453872
- PMCID: PMC8652989
- DOI: 10.1111/ajt.16818
Cellular immunity predominates over humoral immunity after homologous and heterologous mRNA and vector-based COVID-19 vaccine regimens in solid organ transplant recipients
Abstract
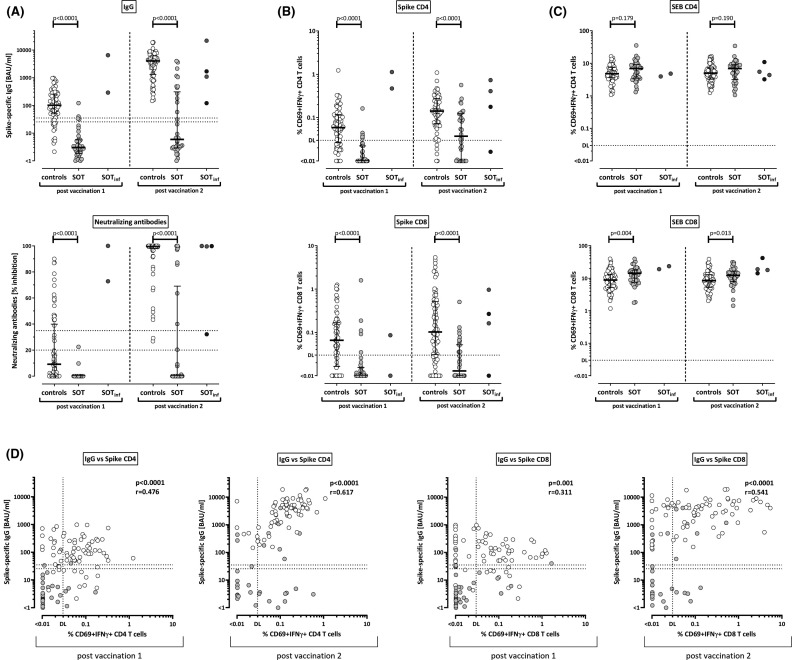
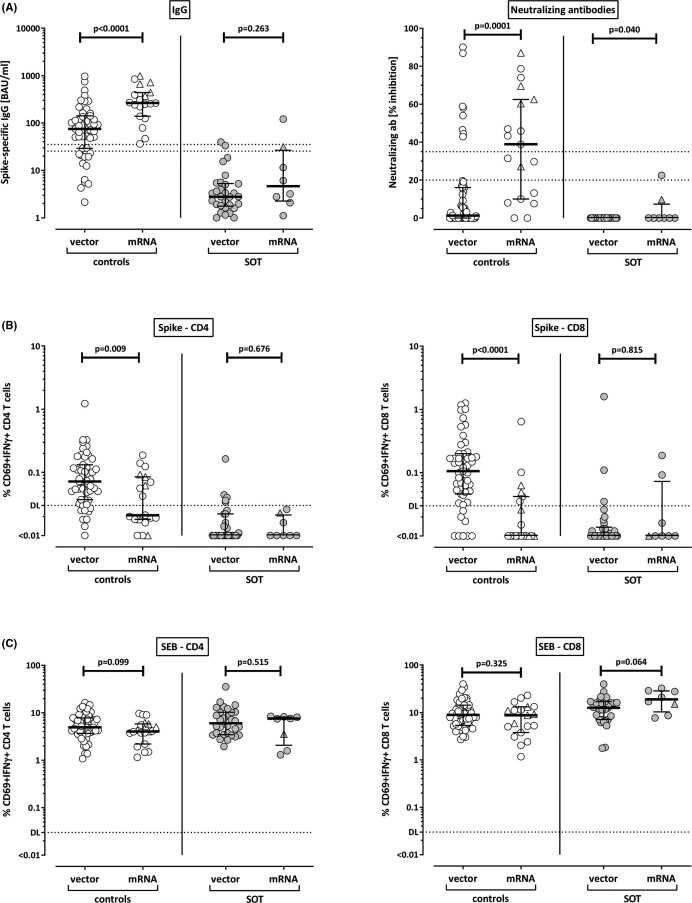
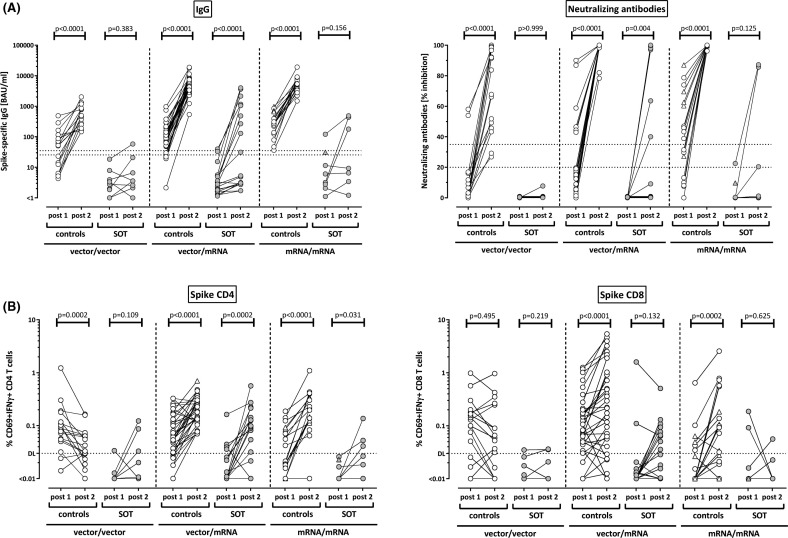
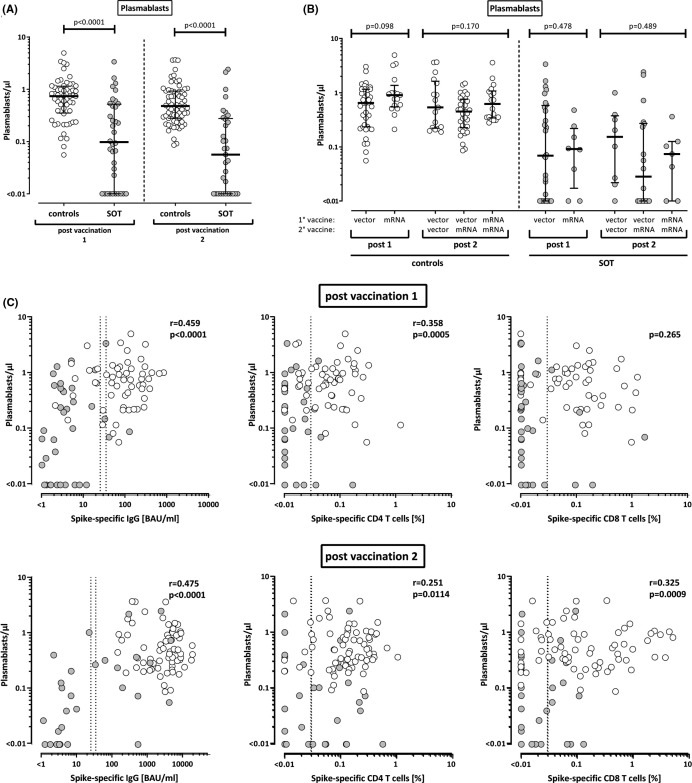
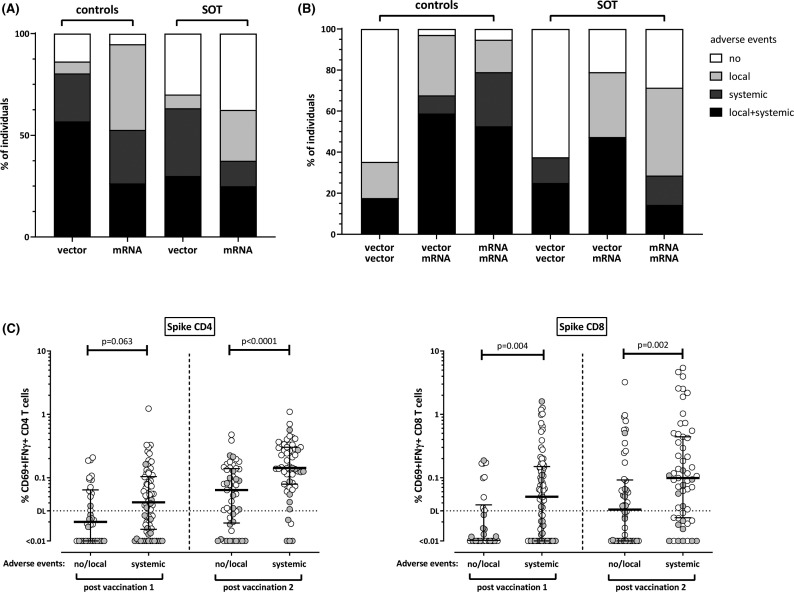
Knowledge on the immunogenicity of vector-based and mRNA-vaccines in solid organ transplant recipients is limited. Therefore, SARS-CoV-2-specific T cells and antibodies were analyzed in 40 transplant recipients and 70 controls after homologous or heterologous vaccine-regimens. Plasmablasts and SARS-CoV-2-specific CD4 and CD8 T cells were quantified using flow cytometry. Specific antibodies were analyzed by ELISA and neutralization assay. The two vaccine types differed after the first vaccination, as IgG and neutralizing activity were more pronounced after mRNA priming (p = .0001 each), whereas CD4 and CD8 T cell levels were higher after vector priming (p = .009; p = .0001). All regimens were well tolerated, and SARS-CoV-2-specific antibodies and/or T cells after second vaccination were induced in 100% of controls and 70.6% of transplant recipients. Although antibody and T cell levels were lower in patients, heterologous vaccination led to the most pronounced induction of antibodies and CD4 T cells. Plasmablast numbers were significantly higher in controls and correlated with SARS-CoV-2-specific IgG- and T cell levels. While antibodies were only detected in 35.3% of patients, cellular immunity was more frequently found (64.7%) indicating that assessment of antibodies is insufficient to identify COVID-19-vaccine responders. In conclusion, heterologous vaccination seems promising in transplant recipients, and combined analysis of humoral and cellular immunity improves the identification of responders among immunocompromised individuals.
Keywords: T cell biology; clinical research/practice; flow cytometry; infection and infectious agents - viral; infectious disease; vaccine.
© 2021 The Authors. American Journal of Transplantation published by Wiley Periodicals LLC on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
