

Clustering and multiple-spreading events of nosocomial severe acute respiratory syndrome coronavirus 2 infection
- PMID: 34453983
- PMCID: PMC8384763
- DOI: 10.1016/j.jhin.2021.06.012
Clustering and multiple-spreading events of nosocomial severe acute respiratory syndrome coronavirus 2 infection
Abstract
Background: There is growing evidence that super-spreading events (SSEs) and multiple-spreading events (MSEs) are a characteristic feature of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. However, data regarding the possibility of SSEs or MSEs in healthcare settings are limited.
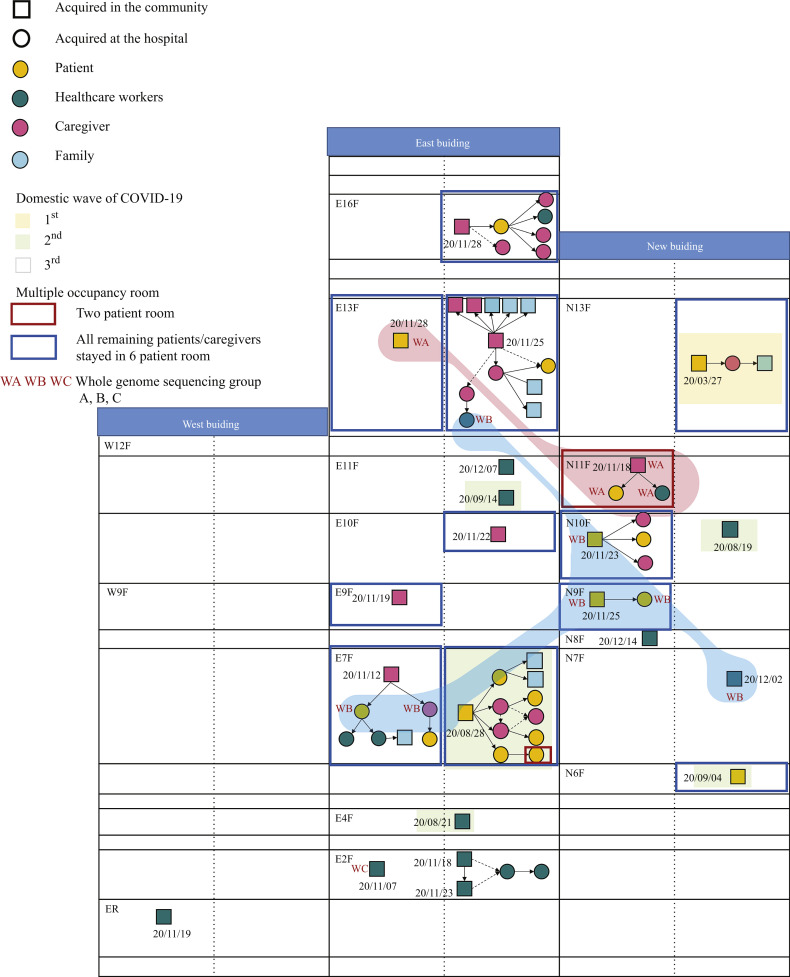
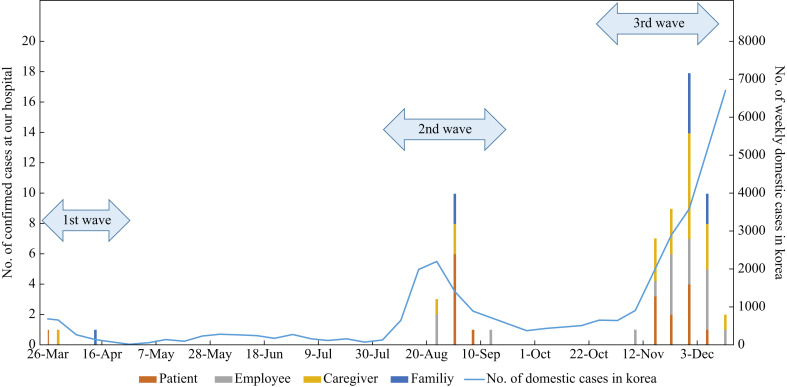
Methods: This study was performed at a tertiary-care hospital in Korea. We analysed the nosocomial COVID-19 cases that occurred in healthcare workers and inpatients and their caregivers between January and 20th December 2020. Cases with two to four secondary cases were defined as MSEs and those with five or more secondary cases as SSEs.
Findings: We identified 21 nosocomial events (single-case events, N = 12 (57%); MSE + SSE, N = 9 (43%)) involving 65 individuals with COVID-19. Of these 65 individuals, 21 (32%) were infectors. The infectors tended to have a longer duration between symptom onset and diagnostic confirmation than did the non-infectors (median two days vs zero days, P=0.08). Importantly, 12 (18%) individuals were responsible for MSEs and one (2%) for an SSE, which collectively generated 35 (54%) secondary cases.
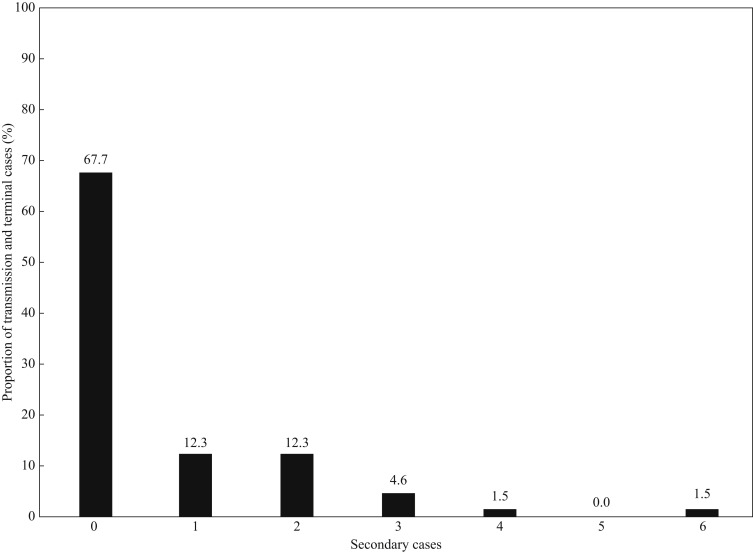
Conclusion: In a hospital with thorough infection-control measures, approximately 70% of the nosocomial cases of COVID-19 did not generate secondary cases, and one-fifth of the infectors were responsible for SSEs and MSEs, which accounted for approximately half of the total cases. Early case identification, isolation, and extensive contact tracing are important for the prevention of transmission and SSEs.
Keywords: COVID-19; SARS-CoV-2; Transmission.
Copyright © 2021 The Healthcare Infection Society. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Adam D.C., Wu P., Wong J.Y., Lau E.H., Tsang T.K., Cauchemez S. Clustering and superspreading potential of SARS-CoV-2 infections in Hong Kong. Nature Med. 2020;26:1714–1719. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
