

Regional biomechanical and failure properties of healthy human ascending aorta and root
- PMID: 34454207
- PMCID: PMC8513753
- DOI: 10.1016/j.jmbbm.2021.104705
Regional biomechanical and failure properties of healthy human ascending aorta and root
Abstract
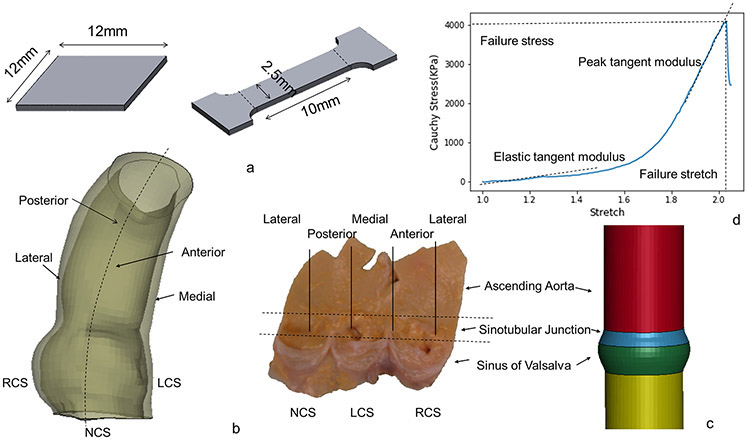
Purpose: Aortic dissection (AD) is a life-threatening event that occurs when the intimal entry tear propagates and separates inner from outer layers of the aorta. Diameter, the current criterion for aneurysm repair, is far from ideal and additional evidence to optimize clinical decision would be extremely beneficial. Biomechanical investigation of the regional failure properties of aortic tissue is essential to understand and proactively prevent AD. We previously studied biaxial mechanical properties of healthy human aorta. In this study, we investigated the regional failure properties of healthy human ascending aorta (AscAo) including sinuses of Valsalva (SOV), and sinotubular junction (STJ).
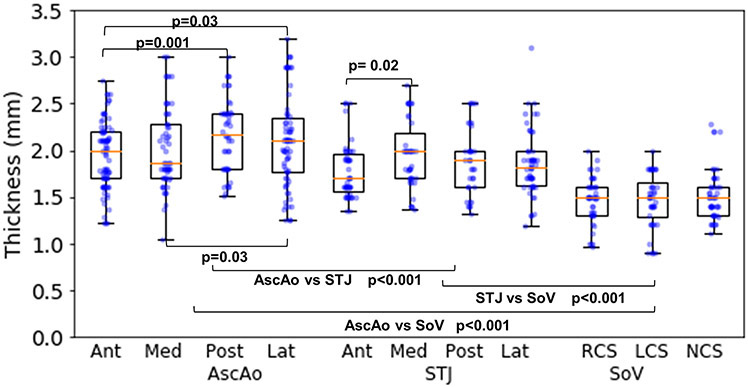
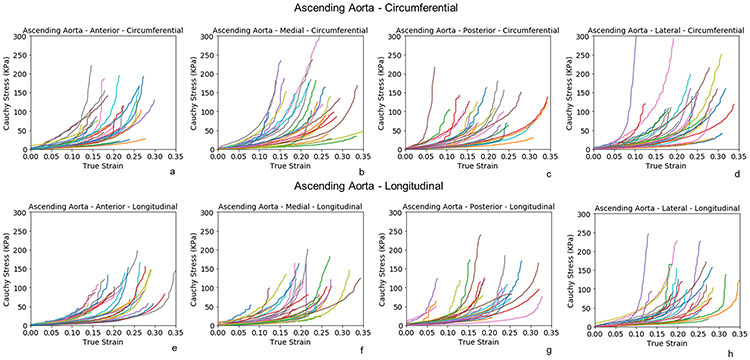
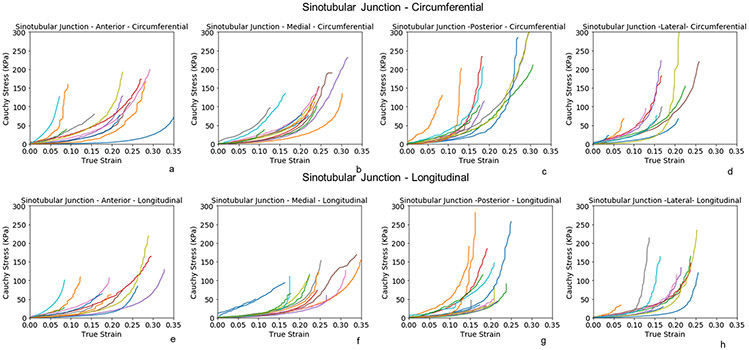
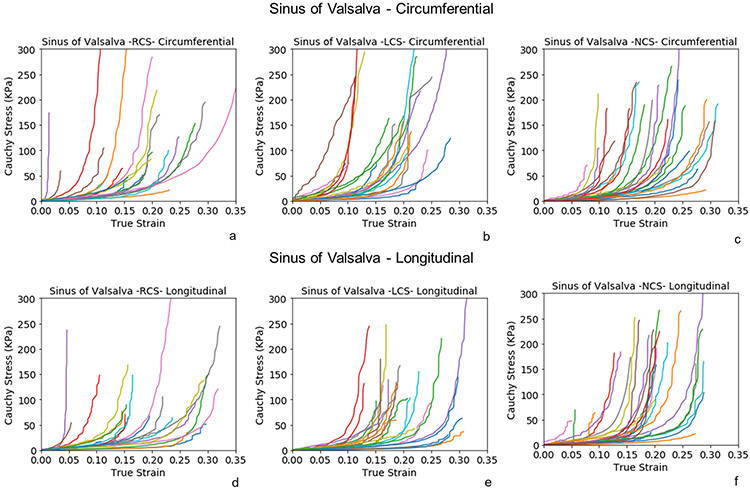
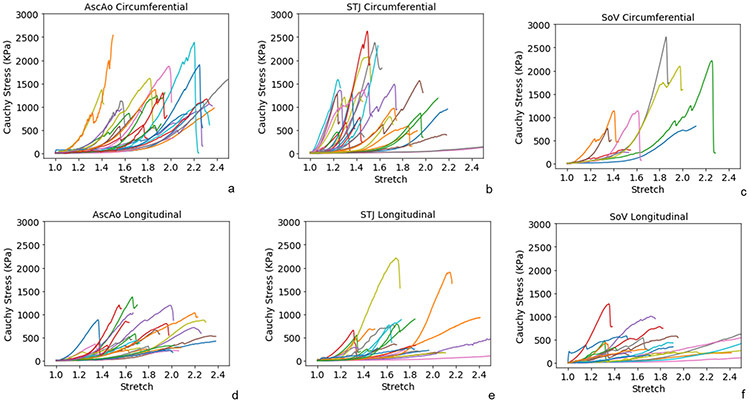
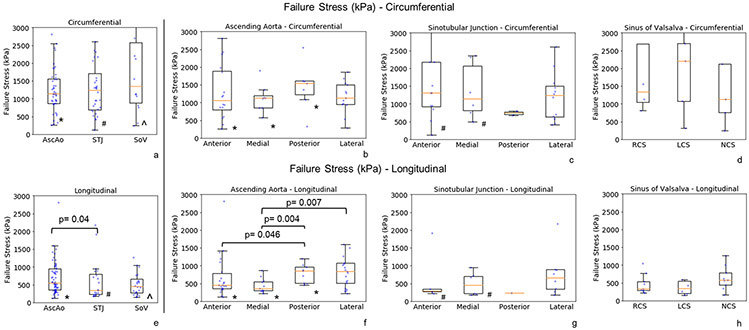
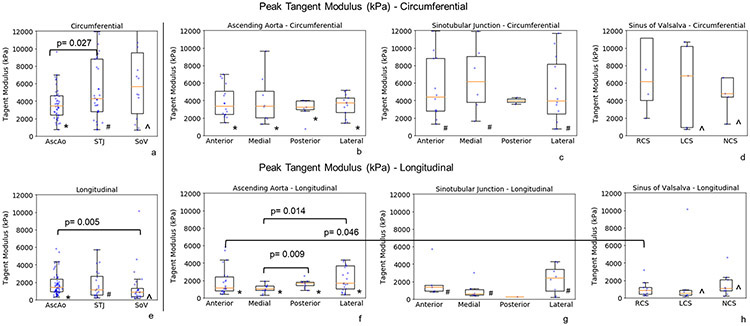
Results: A total of 430 intact tissue samples were harvested from 19 healthy donors whose hearts were excluded from heart transplantation. The donors had mean age of 51 ± 11.7 years and nearly equal gender distribution. Samples were excised from aortic regions and subregions at defined locations. Tissue strips were subjected to either biaxial or uniaxial failure testing. Wall thickness varied regionally being thickest at AscAo (2.08 ± 0.66 mm) and thinnest at SOV (1.46 ± 0.31 mm). Biaxial testing demonstrated hyperplastic behavior of aortic tissues. Posterior and lateral STJ subregions were found to be stiffer than anterior and medial subregions in both circumferential and longitudinal directions. Failure stresses were significantly higher in the circumferential than longitudinal directions in each subregion of AscAo, STJ, and SOV. Longitudinal failure stresses were significantly greater in AscAo than those in STJ or SOV. Longitudinal failure stresses in AscAo were much smaller anteriorly than posteriorly, and medially than laterally.
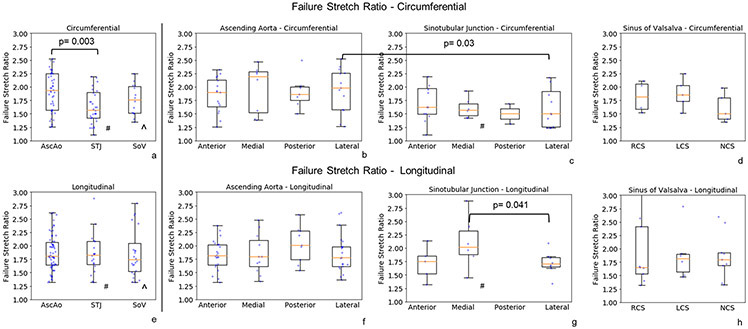
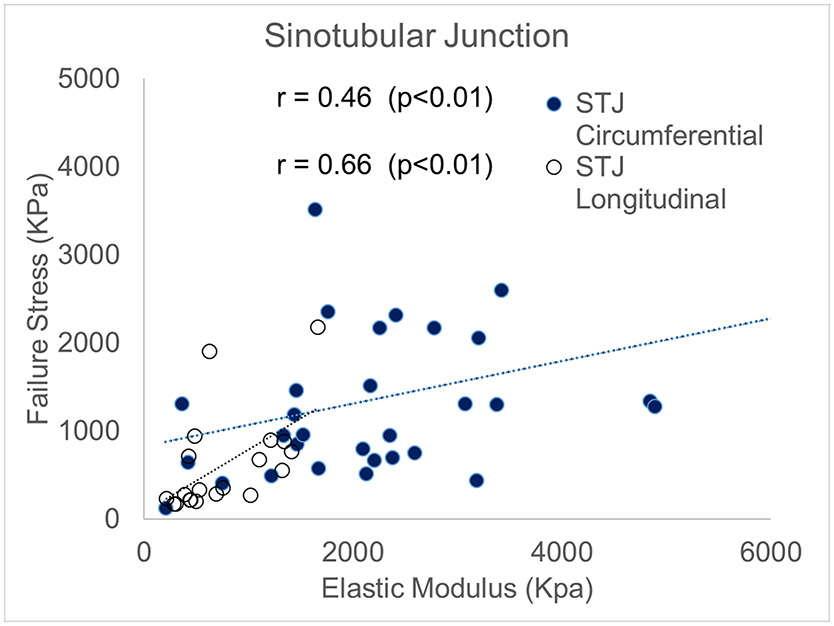
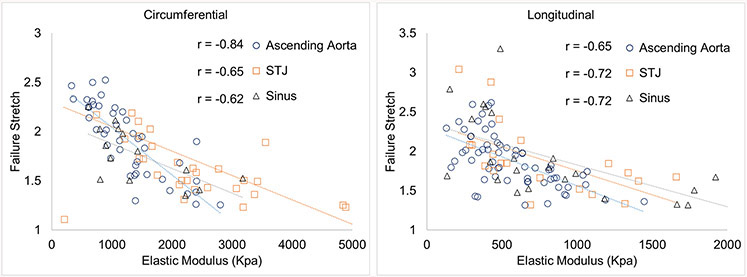
Conclusions: The finding of weakest region at the sinotubular junction along the longitudinal direction corroborates clinical observations of that region being commonly involved as the initial site of intimal tear in aortic dissections. Failure stretch ratios correlated to elastic modulus at each region. Furthermore, strong correlation was seen between STJ failure stresses and elastic modulus at physiological pressure along both circumferential and longitudinal directions. Correlating in-vivo aortic elastic modulus based on in-vivo imaging with experimentally determined elastic modulus at physiological pressure and failure stresses may potentially provide valuable information regarding aortic wall strength. Better understanding of aortic biomechanics in normal physiologic and aneurysmal pathologic states may aid in determining risk factors for predicting dissection in patient-specific fashion.
Keywords: Aortic dissection; Ascending aorta; Biaxial; Biomechanics; Failure stress; Healthy; Peak tangent modulus; Stretch.
Copyright © 2021. Published by Elsevier Ltd.
Conflict of interest statement
Figures
References
-
- Azadani AN, Chitsaz S, Mannion A, Mookhoek A, Wisneski A, Guccione JM, Hope MD, Ge L, Tseng EE, 2013. Biomechanical properties of human ascending thoracic aortic aneurysms. Ann Thorac Surg 96, 50–58. - PubMed
-
- Azadani AN, Chitsaz S, Matthews PB, Jaussaud N, Leung J, Tsinman T, Ge L, Tseng EE, 2012a. Comparison of mechanical properties of human ascending aorta and aortic sinuses. Ann Thorac Surg 93, 87–94. - PubMed
-
- Azadani AN, Chitsaz S, Matthews PB, Jaussaud N, Leung J, Wisneski A, Ge L, Tseng EE, 2012b. Biomechanical comparison of human pulmonary and aortic roots. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery 41, 1111–1116. - PubMed
-
- Cacho F, Elbischger PJ, Rodríguez JF, Doblaré M, Holzapfel GA, 2007. A constitutive model for fibrous tissues considering collagen fiber crimp. International Journal of Non-Linear Mechanics 42, 391–402.
-
- Choudhury N, Bouchot O, Rouleau L, Tremblay D, Cartier R, Butany J, Mongrain R, Leask RL, 2009. Local mechanical and structural properties of healthy and diseased human ascending aorta tissue. Cardiovascular Pathology 18, 83–91. - PubMed
