

Patient-reported outcomes in coronary artery disease: the relationship between the standard, disease-specific set by the International Consortium for Health Outcomes Measurement (ICHOM) and the generic health-related quality of life instrument 15D
- PMID: 34454528
- PMCID: PMC8401180
- DOI: 10.1186/s12955-021-01841-6
Patient-reported outcomes in coronary artery disease: the relationship between the standard, disease-specific set by the International Consortium for Health Outcomes Measurement (ICHOM) and the generic health-related quality of life instrument 15D
Abstract
Background: Patient-reported outcome (PRO) instruments measure health gains, including changes in health-related quality of life (HRQoL). Previous studies have assessed the reliability and relationship of multiple HRQoL instruments in search of the optimal instrument for feasible measurement of PROs. Although the 15D instrument was shown to have the best sensitivity and construct validity among cardiac patients, it is unknown how well it captures relevant disease-specific information scores compared to instruments included in the International Consortium for Health Outcomes Measurement (ICHOM) standard set. The aim of this study was to investigate whether the disease-specific PRO instruments and a generic HRQoL instrument capture disease related symptoms in coronary artery disease (CAD) patients.
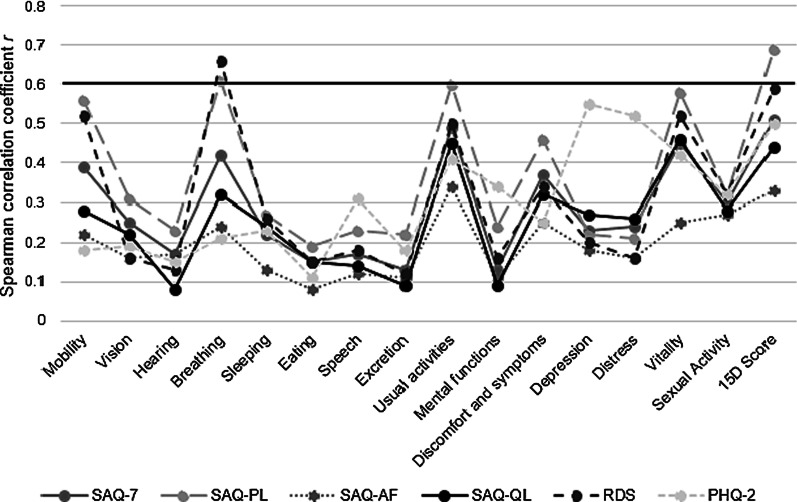
Methods: Health status and HRQoL were assessed with the instruments included in the ICHOM standard set: Seattle Angina Questionnaire short-form (SAQ-7), Rose Dyspnea Scale (RDS), two-item Patient Health Questionnaire (PHQ-2), and with the 15D HRQoL instrument at baseline and 1 year from the treatment in a university hospital setting. Spearman correlation and explanatory factor analysis were used to assess the relationship of baseline scores and 1-year change in scores of 297 patients.
Results: At baseline, the overall 15D score and SAQ-physical limitation (SAQ-PL), 15D "breathing" and SAQ-PL, as well as "breathing" and RDS showed moderately strong correlations. The factor interpreted to reflect "Breathing-related physical activity", based on high loadings of "breathing", RDS, SAQ-PL, "mobility", "vitality", and "usual activities", explained 19.2% of the total variance. Correlations between 1-year changes in scores were fair. The factor of "Breathing-related physical activity", with significant loading of RDS, SAQ-PL, "breathing, "usual activities", "vitality", "sexual activity", "mobility", and disease-specific quality of life explained 20.5% of the total variance in 1-year change in scores. The correlation of angina frequency measured by SAQ-7 and the 15D instrument was poor.
Conclusions: The 15D detects dyspnea and depression similarly to RDS and PHQ-2 but not angina similarly to the SAQ-7. This may call for supplementing the 15D instrument with a disease-specific instrument when studying CAD patients.
Keywords: Coronary artery disease; Health status assessment; Health-related quality of life; Patient-reported outcomes.
© 2021. The Author(s).
Conflict of interest statement
JM is a founding partner of ESiOR—Expert Solutions in Outcomes Research Ltd. and a board member of Siltana Ltd. These companies were not involved in carrying out this research. HS is the developer of the 15D and obtains from its electronic versions.
Figures
Similar articles
-
Correlation of the disease-specific Canadian Cardiovascular Society (CCS) classification and health-related quality of life (15D) in coronary artery disease patients.PLoS One. 2022 Apr 1;17(4):e0266101. doi: 10.1371/journal.pone.0266101. eCollection 2022. PLoS One. 2022. PMID: 35363816 Free PMC article.
-
Standardized Outcome Measurement for Patients With Coronary Artery Disease: Consensus From the International Consortium for Health Outcomes Measurement (ICHOM).J Am Heart Assoc. 2015 May 19;4(5):e001767. doi: 10.1161/JAHA.115.001767. J Am Heart Assoc. 2015. PMID: 25991011 Free PMC article.
-
Comparison between the disease-specific Airways Questionnaire 20 and the generic 15D instruments in COPD.Health Qual Life Outcomes. 2011 Jan 16;9:4. doi: 10.1186/1477-7525-9-4. Health Qual Life Outcomes. 2011. PMID: 21235818 Free PMC article.
-
Interpretation of the Seattle Angina Questionnaire as an Outcome Measure in Clinical Trials and Clinical Care: A Review.JAMA Cardiol. 2021 May 1;6(5):593-599. doi: 10.1001/jamacardio.2020.7478. JAMA Cardiol. 2021. PMID: 33566062 Free PMC article. Review.
-
Measurement of dyspnea and quality of life in advanced lung disease.Clin Chest Med. 1997 Sep;18(3):457-69. doi: 10.1016/s0272-5231(05)70394-4. Clin Chest Med. 1997. PMID: 9329869 Review.
Cited by
-
Potentially inappropriate medication use and comorbidity in association with quality of life in community-dwelling older people: a cross-sectional study in Iran.BMC Prim Care. 2025 May 20;26(1):175. doi: 10.1186/s12875-025-02882-2. BMC Prim Care. 2025. PMID: 40394468 Free PMC article.
-
Depressive symptoms decrease health-related quality of life of patients with coronary artery disease and diabetes: a 12-month follow up study in primary care.Scand J Prim Health Care. 2023 Sep;41(3):276-286. doi: 10.1080/02813432.2023.2233995. Epub 2023 Jul 16. Scand J Prim Health Care. 2023. PMID: 37455531 Free PMC article. Clinical Trial.
References
-
- Ulvik B, Bjelland I, Hanestad BR, Omenaas E, Wentzel-Larsen T, Nygard O. Comparison of the Short Form 36 and the Hospital Anxiety and Depression Scale measuring emotional distress in patients admitted for elective coronary angiography. Heart Lung. 2008;37:286–295. doi: 10.1016/j.hrtlng.2007.08.001. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
