

Neuro-ophthalmologic outcomes of standard versus hypo-fractionated stereotactic radiotherapy of AVPM
- PMID: 34454551
- PMCID: PMC8403384
- DOI: 10.1186/s13014-021-01879-2
Neuro-ophthalmologic outcomes of standard versus hypo-fractionated stereotactic radiotherapy of AVPM
Abstract
Background: Most anterior visual pathway meningiomas (AVPM) are benign and slow-growing, but these tumors may affect visual functions, including visual acuity (VA) and visual field (VF). Due to location, most are treated non-surgically by fractionated stereotactic radiotherapy (FSRT), aiming to prevent tumor progression and visual functions deterioration. Unfortunately, FSRT in itself may affect visual functions. The current preferred treatment regimen (in terms of safety and effectiveness) is undetermined. While most cases are treated with conventional fractionation (cFSRT)-50.4-54 Gy in 28-30 fractions of 1.8-2 Gy, advances in technology have allowed shortening of total treatment length to hypofractionation (hSRT)-25-27 Gy in 3-5 fractions of 5-9 Gy. Our aim was to evaluate the association of radiotherapy regimen for treating AVPM (cFSRT vs. hSRT) with visual function outcomes (VA, VF) at the last neuro-ophthalmologic evaluation.
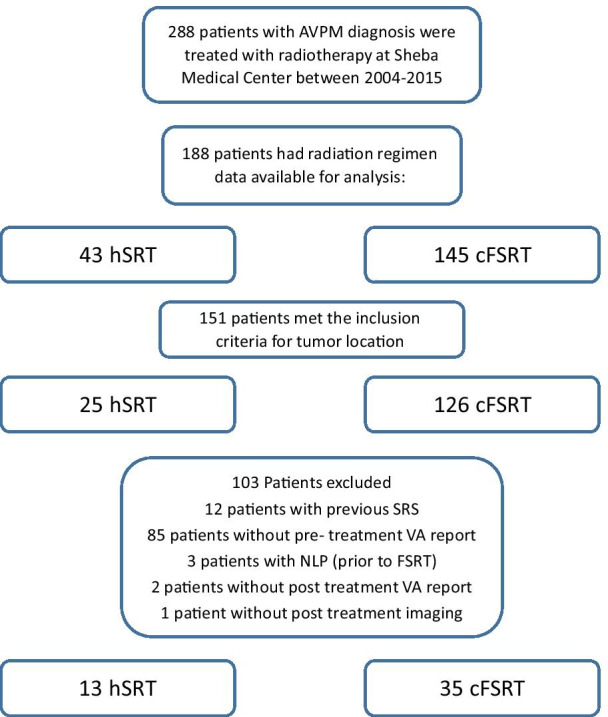
Methods: We conducted a retrospective cohort study of AVPM cases treated at Sheba Medical Center during 2004-2015. We compared cFSRT and hSRT regimens regarding visual function (VA, VF) outcomes at the last neuro-ophthalmologic evaluation. VA was determined by the logarithm of the minimum angle of resolution (LogMAR). VF was determined by the mean deviation (MD). A clinically relevant change in VA was defined as 0.2 LogMAR.
Results: 48 patients (13 receiving hSRT, 35 receiving cFSRT) were included, with a median follow-up of 55 months. No significant difference was evident regarding LogMAR or MD of involved eyes at the last evaluation. Six (17%) patients in the cFSRT group experienced clinically relevant VA deterioration in the involved eye, compared with six (46%) in hSRT (p = 0.06).
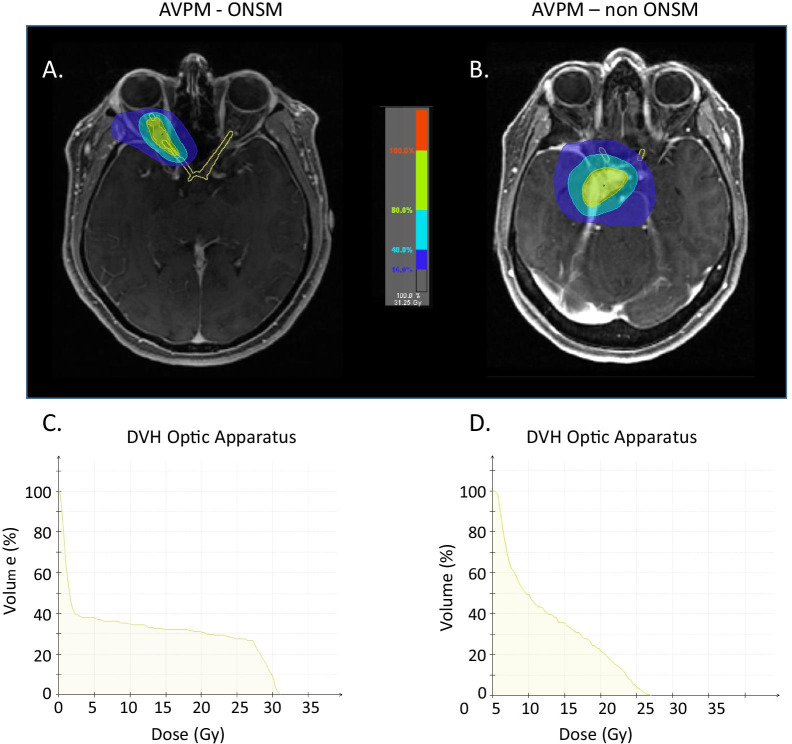
Conclusion: Our findings, using comprehensive and meticulous investigation of visual outcomes, suggest that hSRT may be associated with higher risk for VA and VF deterioration in AVPM especially in ONSM. We recommend the use of cFSRT for ONSM.
© 2021. The Author(s).
Conflict of interest statement
All authors declare they have no competing interests.
Figures
References
-
- Kansu T. Neuro-ophthalmology of Meningiomas. In: Pamir MN, Black PM, Fahlbusch R, eds. Meningiomas. Elsevier; 2010:177–189. 10.1016/B978-1-4160-5654-6.00012-X.
-
- Pamir MN, Black PM, Fahlbusch R. CHAPTER 18—decision making in meningiomas. In: Pamir MN, Black PM, Fahlbusch R, eds. Meningiomas. W.B. Saunders; 2010:275–289. 10.1016/B978-1-4160-5654-6.00018-0.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
