

The impact of physical training on length of hospital stay and physical function in patients hospitalized with community-acquired pneumonia: protocol for a randomized controlled trial
- PMID: 34454594
- PMCID: PMC8397876
- DOI: 10.1186/s13063-021-05503-2
The impact of physical training on length of hospital stay and physical function in patients hospitalized with community-acquired pneumonia: protocol for a randomized controlled trial
Abstract
Background: Community-acquired pneumonia (CAP) is a leading cause of hospitalization worldwide. Bed rest with low levels of physical activity is common during periods of hospitalization and leads to functional decline as well as increased risk of complications. The aim of this study is to assess the effect of supervised physical training during hospitalization with CAP compared with standard usual care for CAP on length of hospital stay, risk of readmission, mortality risk, physical capacity, muscle and fat mass, muscle strength, metabolic function, systemic inflammation, health-related quality of life, and physical activity level.
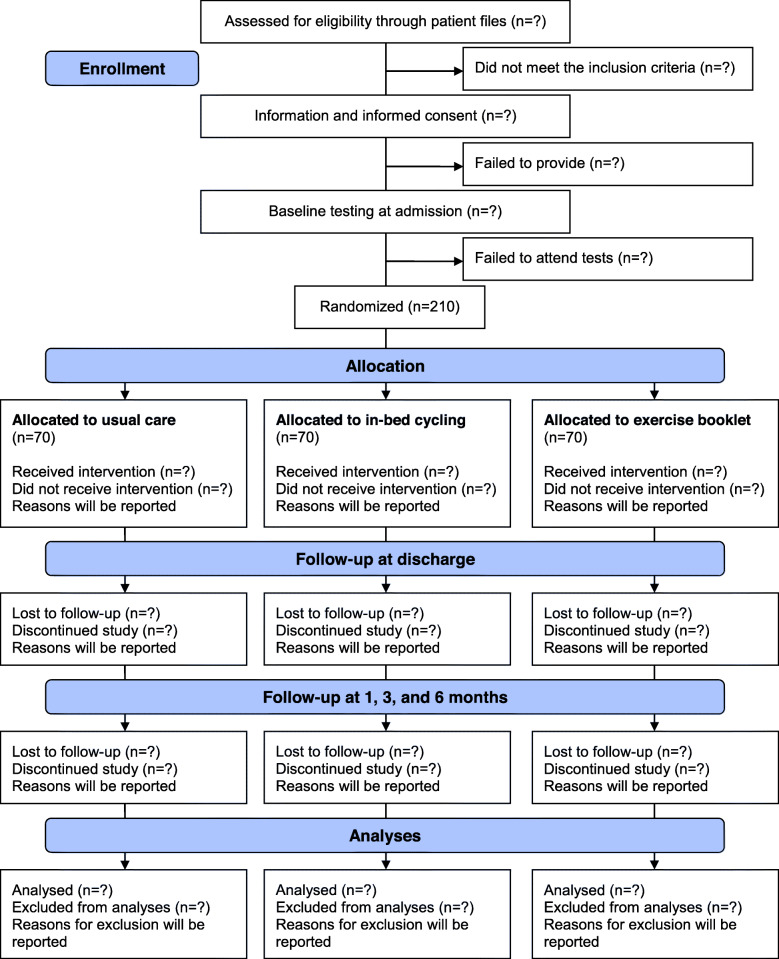
Methods: This study is a randomized controlled trial with three parallel experimental arms. Based on a sample size calculation, a total of 210 patients admitted with CAP at Nordsjællands Hospital, Hillerød, Denmark, will be recruited. Patients will be randomly allocated (1:1:1) to either (1) standard usual care, (2) standard usual care combined with in-bed cycling, or (3) standard usual care combined with exercises from a booklet. The primary outcome is differences in length of hospital stay between groups, with secondary outcomes being differences between groups in time to (1) 90-day readmission and (2) 180-day mortality. Further secondary outcomes are differences in changes from baseline between groups in (3) lean mass, (4) fat mass, (5) fat-free mass, (6) physical capacity, (7) health-related quality of life, (8) systemic inflammation, and (9) physical activity level after discharge. Data on length of hospital stay, readmission, and mortality will be collected from patient files, while total lean, fat, and fat-free mass will be quantitated by dual-energy x-ray absorptiometry and bioelectrical impedance analysis. Physical function will be assessed using grip strength, 30-s chair stand tests, and Barthel Index-100. Health-related quality of life will be assessed with the EQ-5D-5L questionnaire. Systemic inflammation will be assessed in blood samples, while accelerometers are used for measuring physical activity.
Discussion: If a simple physical training program appears to diminish the impact of critical illness and hospitalization on clinical outcome, mobility, and health-related quality of life, it may lead to novel therapeutic approaches in the treatment of patients hospitalized with CAP.
Trial registration: ClinicalTrials.gov NCT04094636 . Registered on 1 April 2019.
Keywords: Community-acquired pneumonia; Functional ability; Lean mass; Length of hospital stay; Physical training.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, AlMazroa MA, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Abdulhak AB, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, de Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FGR, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Memish ZA, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KMV, Nasseri K, Norman P, O'Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA, III, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, de León FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJL. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Petersen PT, Egelund GB, Jensen AV, Andersen SB, Pedersen MF, Rohde G, Ravn P. Associations between biomarkers at discharge and co-morbidities and risk of readmission after community-acquired pneumonia: a retrospective cohort study. Eur J Clin Microbiol Infect Dis. 2018;37(6):1103–1111. doi: 10.1007/s10096-018-3224-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
