

Arrhythmic and Mortality Outcomes Among Ischemic Versus Nonischemic Cardiomyopathy Patients Receiving Primary ICD Therapy
- PMID: 34454875
- PMCID: PMC8792162
- DOI: 10.1016/j.jacep.2021.06.020
Arrhythmic and Mortality Outcomes Among Ischemic Versus Nonischemic Cardiomyopathy Patients Receiving Primary ICD Therapy
Abstract
Objectives: This study sought to determine the association of cardiomyopathy etiology with the likelihood of ventricular arrhythmias, appropriate implantable cardioverter-defibrillator (ICD) therapy, and mortality.
Background: There are conflicting data on the benefit of primary prevention ICD therapy in patients with ischemic versus nonischemic cardiomyopathy (ICM/NICM).
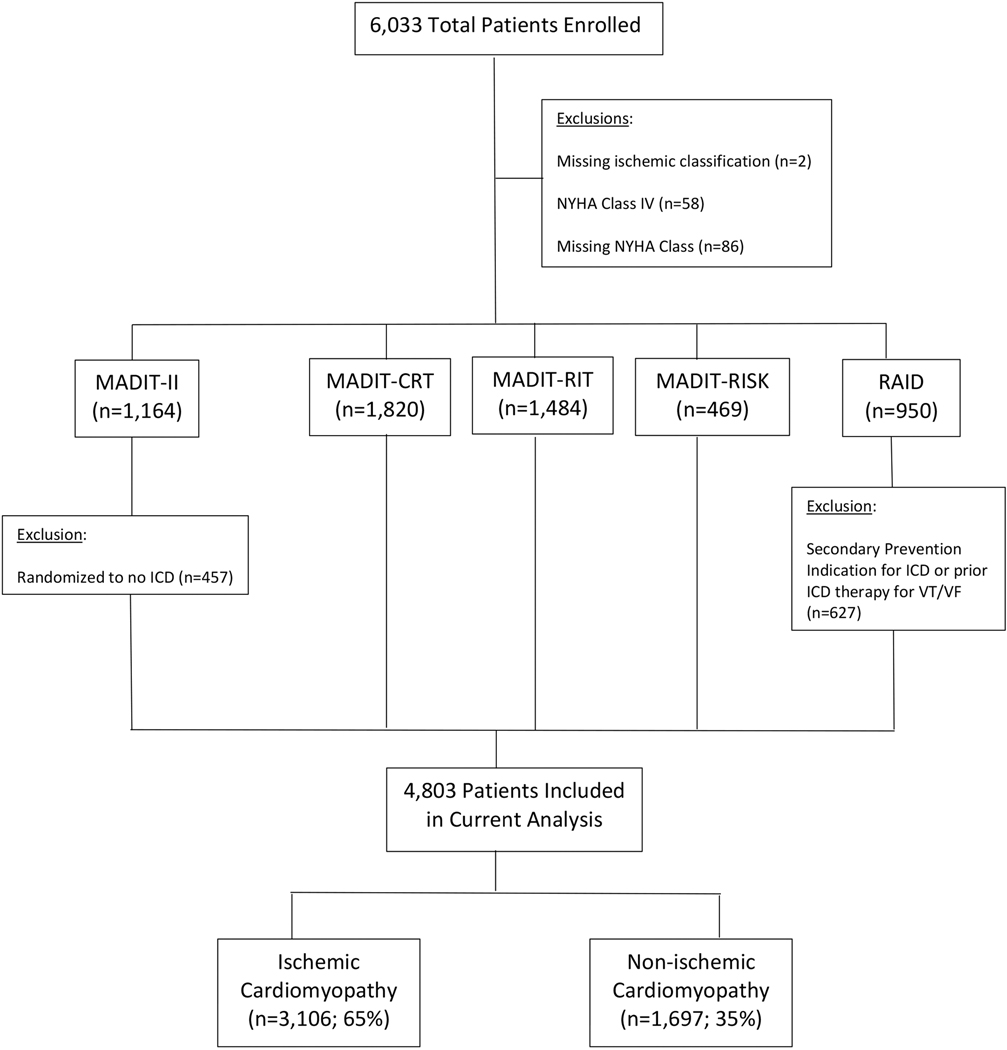
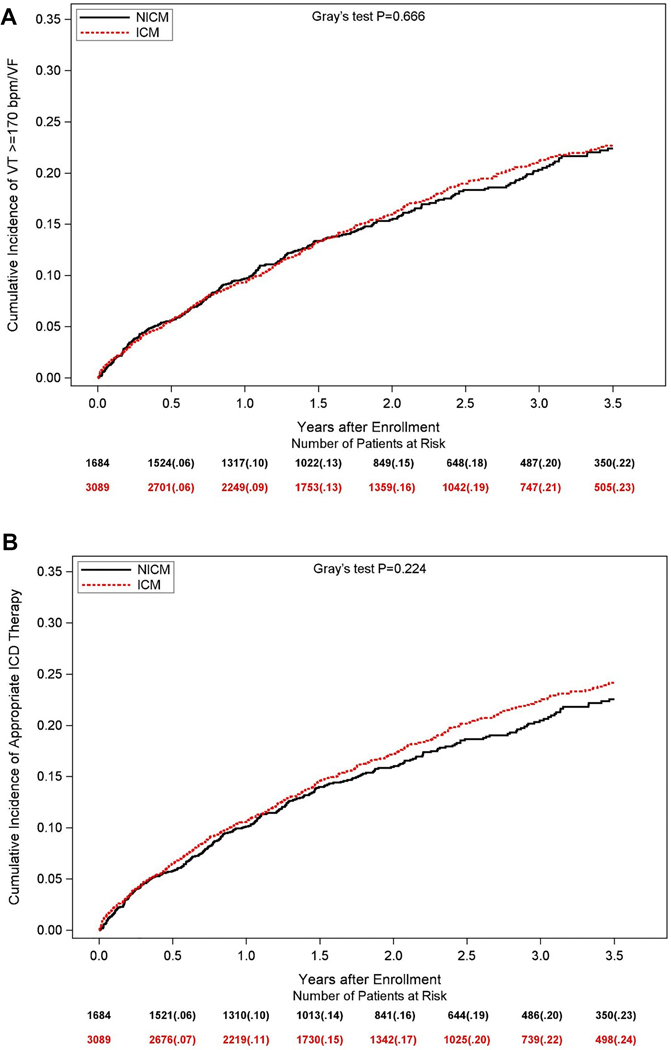
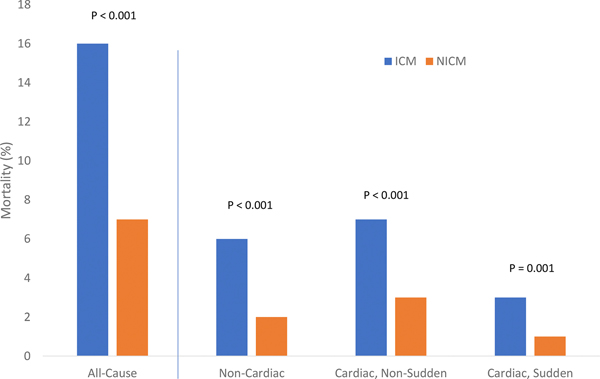
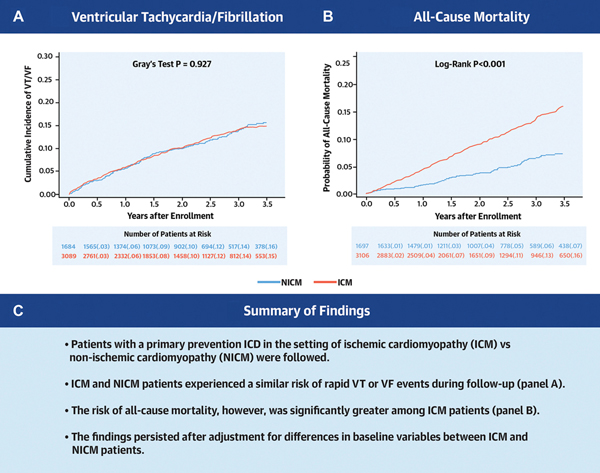
Methods: The study population comprised 4803 patients with ICM (n = 3,106) or NICM (n = 1,697) with a primary prevention ICD enrolled in 5 randomized trials conducted between 1997 and 2017. The primary end point was sustained ventricular tachycardia (VT) ≥200 beats/min or ventricular fibrillation (VF). Secondary end points included appropriate ICD therapy and all-cause mortality. Differences in cause-specific mortality, including noncardiac, sudden cardiac, and non-sudden cardiac death, were also examined.
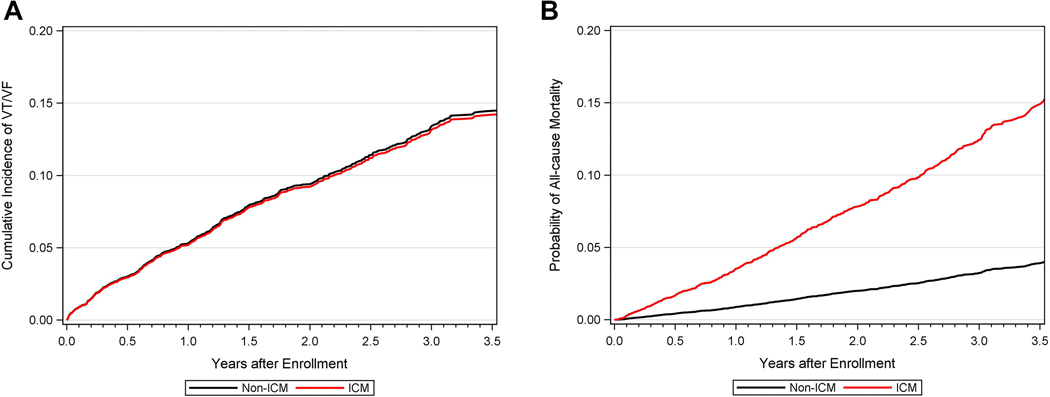
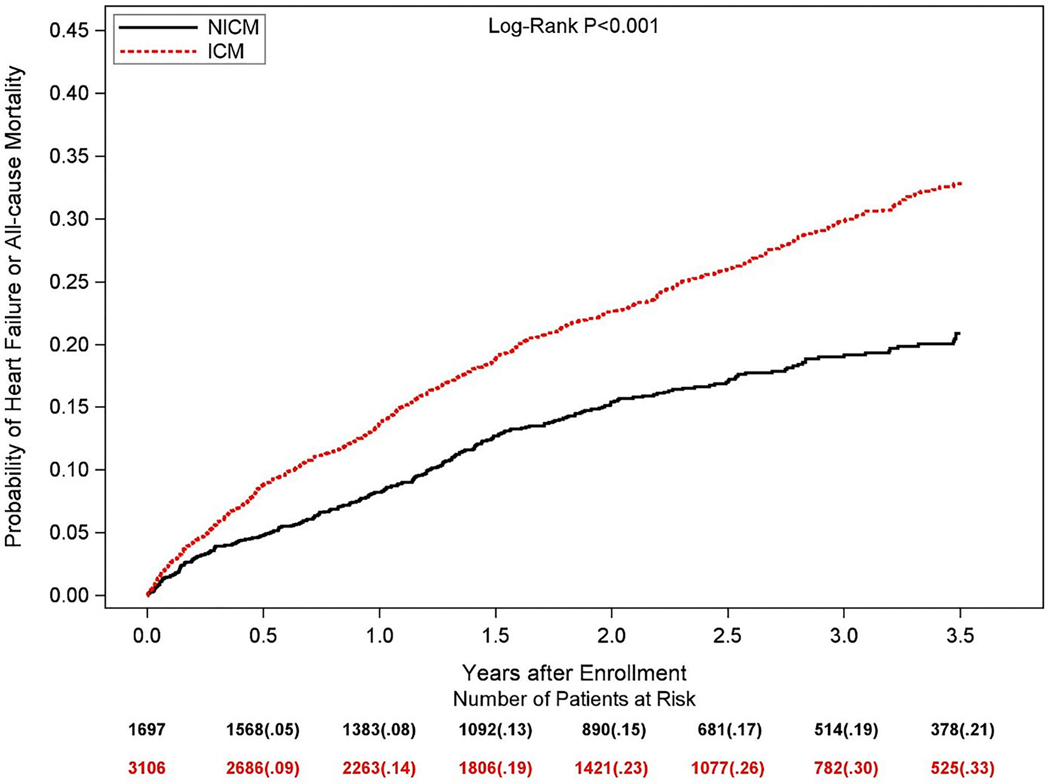
Results: Patients with ICM were significantly older and had more comorbid conditions, whereas those with NICM had a more advanced heart failure class at enrollment and were more often prescribed medical or cardiac resynchronization therapy for heart failure. Multivariate analysis showed that ICM versus NICM had a similar risk of VT/VF events (HR: 0.98 [95% CI: 0.79-1.20]) and appropriate ICD therapy (HR: 1.03 [95% CI: 0.87-1.22]), whereas the risk of all-cause mortality was 1.8-fold higher among ICM versus NICM patients (HR: 1.84 [95% CI: 1.42-2.38]), dominated by non-sudden cardiac mortality.
Conclusions: Combined data from 5 landmark ICD clinical trials show that ICM patients experience a similar risk of life-threatening ventricular arrhythmic events but have an increased risk of all-cause mortality, dominated by non-sudden cardiac death, compared with NICM patients.
Keywords: cardiomyopathies; implantable defibrillators; sudden death; ventricular arrhythmias.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Each of the MADIT trials were funded by an unrestricted research grant from Boston Scientific to the University of Rochester Medical Center, Rochester, NY. The RAID trial was funded by the National Institutes of Health (NIH) grant U01HL096607. Dr Aktas has received research grants from Boston Scientific and Medtronic. Dr Zareba has received research grants from Boston Scientific, LevaNova, Biotronik, and Gilead Sciences; and has been a consultant for Medtronic, Abbott, and Astra-Zeneca. Dr Daubert has received honoraria for serving on events committees, data safety monitoring boards, and advisory boards, as a consultant, and/or for lectures from Abbott, Biosense, Biotronik, Boston Scientific, Farapulse, Medtronic, Microport, Phillips, Vytronus, and Zoll; and has received research grants from Abbott and Medtronic. Dr Huang has received research support from Biosense Webster, Biotronik, and Medtronic; and has received Fellowship Program support from Boston Scientific, Medtronic, Abbott, and Biotronik. Dr Rosero has received research grants from Medtronic, Biotronik, and Spire Inc. Dr Kutyifa has received research grants from Boston Scientific, Biotronik, ZOLL Inc., and Spire Inc.; and has consultant agreements with Zoll Inc. and Biotronik. Dr Goldenberg has received research grants from Boston Scientific, Zoll, Medtronic, Biosense Webster, and Biotronik. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Which Patients Benefit Most From Primary Prevention ICDs?: A Call for More Nuanced Risk Stratification.JACC Clin Electrophysiol. 2022 Jan;8(1):12-14. doi: 10.1016/j.jacep.2021.11.005. JACC Clin Electrophysiol. 2022. PMID: 35057976 No abstract available.
References
-
- Bänsch D, Antz M, Boczor S, et al. Primary prevention of sudden cardiac death in idiopathic dilated cardiomyopathy: the Cardiomyopathy Trial (CAT). Circulation. 2002;105(12):1453–1458. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352(3):225–237. - PubMed
-
- Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350(21):2140–2150. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 1999;341(25):1882–1890. - PubMed
-
- Kadish A, Dyer A, Daubert JP, et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350(21):2151–2158. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
