

Beyond Atherosclerosis and Fibromuscular Dysplasia: Rare Causes of Renovascular Hypertension
- PMID: 34455817
- PMCID: PMC8415524
- DOI: 10.1161/HYPERTENSIONAHA.121.17004
Beyond Atherosclerosis and Fibromuscular Dysplasia: Rare Causes of Renovascular Hypertension
Abstract
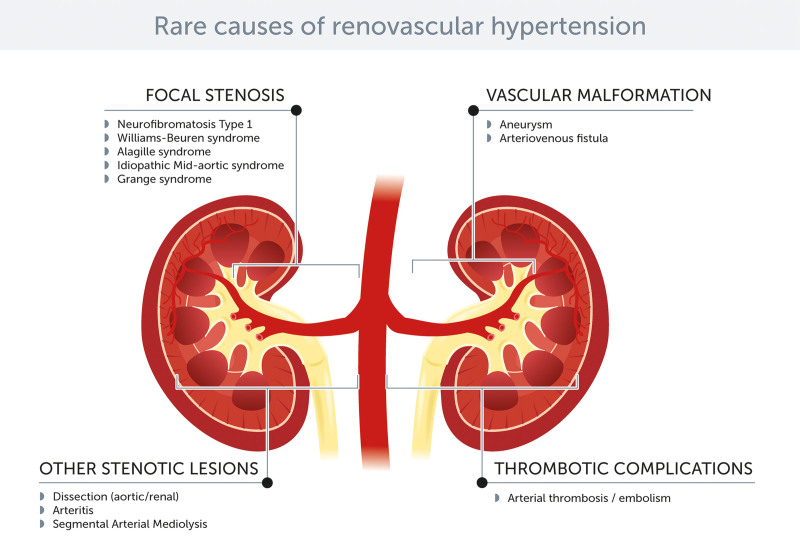
Renovascular hypertension is one of the most common forms of secondary hypertension. Over 95% of cases of renovascular hypertension are due either to atherosclerosis of the main renal artery trunks or to fibromuscular dysplasia. These two causes of renal artery stenosis have been extensively discussed in recent reviews and consensus. The aim of the current article is to provide comprehensive and up-to-date information on the remaining causes. While these causes are rare or extremely rare, etiologic and differential diagnosis matters both for prognosis and management. Therefore, the clinician cannot ignore them. For didactic reasons, we have grouped these different entities into stenotic lesions (neurofibromatosis type 1 and other rare syndromes, dissection, arteritis, and segmental arterial mediolysis) often associated with aortic coarctation and other arterial abnormalities, and nonstenotic lesions, where hypertension is secondary to compression of adjacent arteries and changes in arterial pulsatility (aneurysm) or to the formation of a shunt, leading to kidney ischemia (arteriovenous fistula). Finally, thrombotic disorders of the renal artery may also be responsible for renovascular hypertension. Although thrombotic/embolic lesions do not represent primary vessel wall disease, they are characterized by frequent macrovascular involvement. In this review, we illustrate the most characteristic aspects of these different entities responsible for renovascular hypertension and discuss their prevalence, pathophysiology, clinical presentation, management, and prognosis.
Keywords: aneurysm; arteriovenous fistula; dissection; hypertension, renovascular; neurofibromatosis 1.
Figures
Similar articles
-
Resistant Renovascular Hypertension in Youth: Fibromuscular Dysplasia or Takayasu Arteritis?Am J Case Rep. 2025 Jan 21;26:e945673. doi: 10.12659/AJCR.945673. Am J Case Rep. 2025. PMID: 39834060 Free PMC article.
-
Endovascular interventions in main renal artery pathologies: an overview and update.Acta Radiol. 2022 Jul;63(7):964-975. doi: 10.1177/02841851211019806. Epub 2021 Jun 9. Acta Radiol. 2022. PMID: 34107749 Review.
-
Segmental arterial mediolysis: angioplasty of bilateral renal artery stenoses with 2-year imaging follow-up.J Vasc Interv Radiol. 2004 Jul;15(7):763-7. doi: 10.1097/01.rvi.0000133543.32123.dc. J Vasc Interv Radiol. 2004. PMID: 15231892
-
Fibromuscular dysplasia of the renal arteries.Curr Hypertens Rep. 1999 Dec;1(6):546-9. doi: 10.1007/s11906-996-0028-5. Curr Hypertens Rep. 1999. PMID: 10981119
-
Renovascular Disease and Mesenteric Vascular Disease.Cardiol Clin. 2021 Nov;39(4):527-537. doi: 10.1016/j.ccl.2021.06.005. Cardiol Clin. 2021. PMID: 34686265 Review.
Cited by
-
Resistant Renovascular Hypertension in Youth: Fibromuscular Dysplasia or Takayasu Arteritis?Am J Case Rep. 2025 Jan 21;26:e945673. doi: 10.12659/AJCR.945673. Am J Case Rep. 2025. PMID: 39834060 Free PMC article.
-
Self-limited Hypertension Due to Kidney Infarction.Kidney Med. 2022 Mar 31;4(5):100454. doi: 10.1016/j.xkme.2022.100454. eCollection 2022 May. Kidney Med. 2022. PMID: 35509677 Free PMC article. No abstract available.
-
Renovascular Compression by the Diaphragmatic Crus: A Case Report.Cureus. 2022 Apr 10;14(4):e24004. doi: 10.7759/cureus.24004. eCollection 2022 Apr. Cureus. 2022. PMID: 35547452 Free PMC article.
-
Management of Renovascular Hypertension and Renal Denervation in Patients with Hypertension: An Italian Nationwide Survey.High Blood Press Cardiovasc Prev. 2024 Sep;31(5):501-512. doi: 10.1007/s40292-024-00668-8. Epub 2024 Sep 18. High Blood Press Cardiovasc Prev. 2024. PMID: 39292380 Free PMC article.
-
Spontaneous coronary artery dissection and fibromuscular dysplasia: insights into recent developments.Front Cardiovasc Med. 2024 May 31;11:1409278. doi: 10.3389/fcvm.2024.1409278. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38883987 Free PMC article. Review.
References
-
- Prince M, Tafur JD, White CJ. When and how should we revascularize patients with atherosclerotic renal artery stenosis? JACC Cardiovasc Interv. 2019;12:505–517. doi: 10.1016/j.jcin.2018.10.023 - PubMed
-
- Gornik HL, Persu A, Adlam D, Aparicio LS, Azizi M, Boulanger M, Bruno RM, de Leeuw P, Fendrikova-Mahlay N, Froehlich J, et al. . First International Consensus on the diagnosis and management of fibromuscular dysplasia. Vasc Med. 2019;24:164–189. doi: 10.1177/1358863X18821816 - PubMed
-
- Pappaccogli M, Di Monaco S, Warchoł-Celińska E, Lorthioir A, Amar L, Aparicio LS, Beauloye C, Bruno RM, Chenu P, de Leeuw P, et al. ; European/International FMD Registry and Initiative (FEIRI), and the Working Group ‘Hypertension and the Kidney’ of the European Society of Hypertension (ESH). The European/International Fibromuscular Dysplasia Registry and Initiative (FEIRI)-clinical phenotypes and their predictors based on a cohort of 1000 patients. Cardiovasc Res. 2021;117:950–959. doi: 10.1093/cvr/cvaa102 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
