

Nomogram for the Prediction of Intrahospital Mortality Risk of Patients with ST-Segment Elevation Myocardial Infarction Complicated with Hyperuricemia: A Multicenter Retrospective Study
- PMID: 34456567
- PMCID: PMC8387320
- DOI: 10.2147/TCRM.S320533
Nomogram for the Prediction of Intrahospital Mortality Risk of Patients with ST-Segment Elevation Myocardial Infarction Complicated with Hyperuricemia: A Multicenter Retrospective Study
Abstract
Purpose: This study aimed to establish an accurate and easy predictive model for ST-segment elevation myocardial infarction (STEMI) patients with hyperuricemia, using readily available features to estimate intrahospital mortality risk.
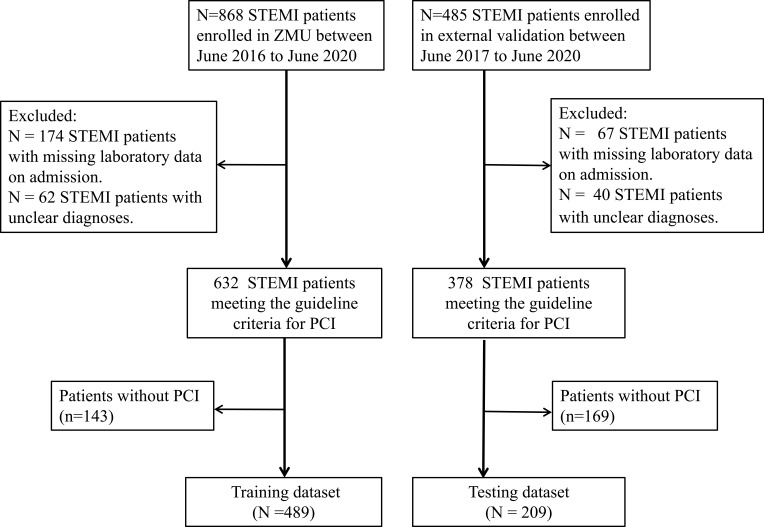
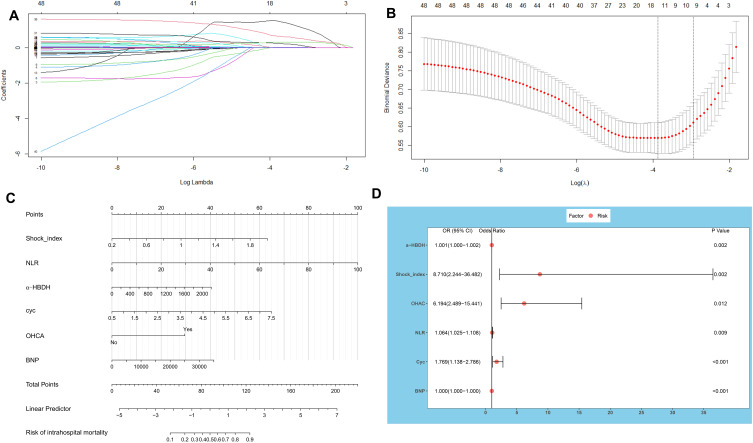
Patients and methods: This was a multicenter retrospective study involving the development of risk prediction models for intrahospital mortality among all STEMI patients with hyperuricemia from Zunyi Medical University Chest Pain Center's specialized alliance between January 1, 2016 and June 30, 2020. The primary outcome was intrahospital mortality. A total of 48 candidate variables were considered from demographic and clinical data. The least absolute shrinkage and selection operator (LASSO) was used to develop a nomogram. Concordance index values, decision curve analysis, the area under the curve (AUC), and clinical impact curves were examined. In this study, 489 patients with STEMI were included in the training dataset and an additional 209 patients from the 44 chest pain centers were included in the test cohort. B-type natriuretic peptides, α-hydroxybutyrate dehydrogenase (α-HBDH), cystatin C, out-of-hospital cardiac arrest (OHCA), shock index, and neutrophil-to-lymphocyte ratio were associated with intrahospital mortality and included in the nomogram.
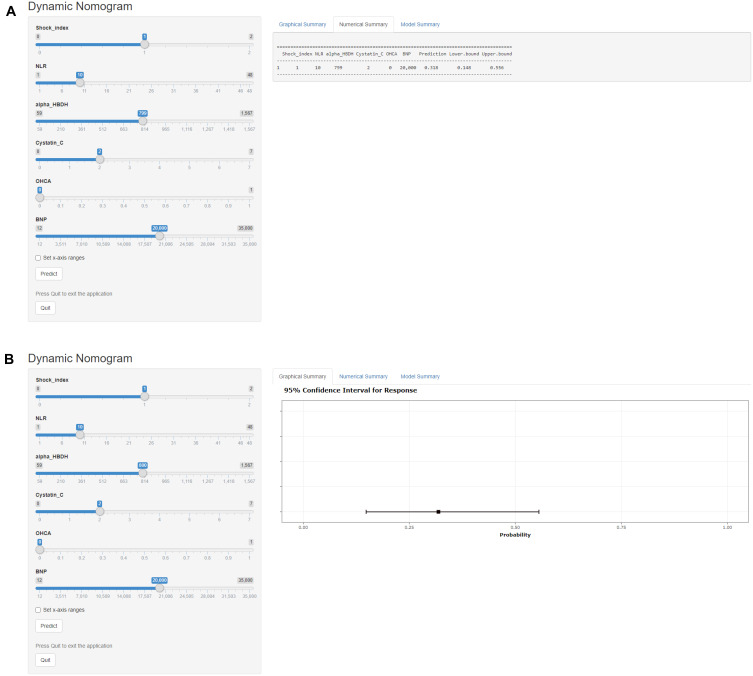
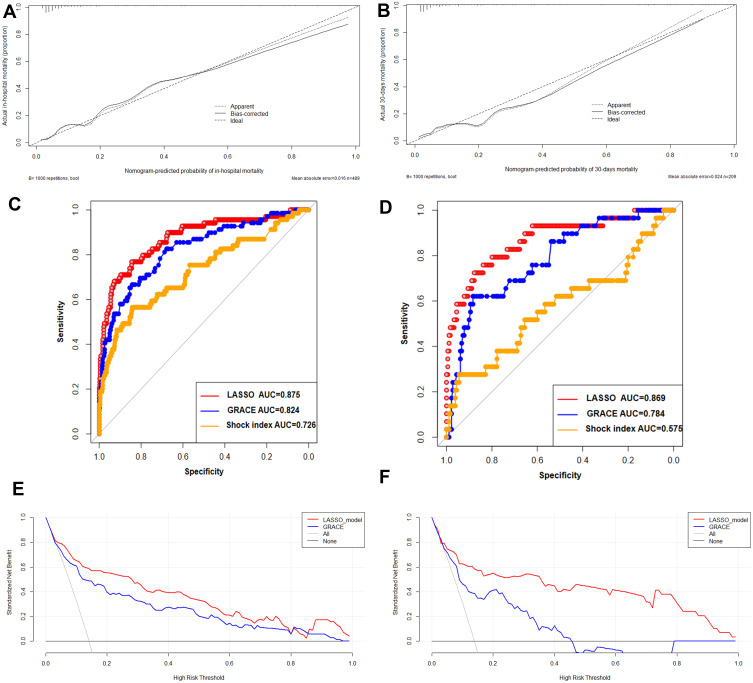
Results: The model showed good discrimination power, and the AUC generated to predict survival in the training set was 0.875 (95% confidence interval, 0.825-0.925). In the validation set, the AUC of survival predictions was 0.87 (95% confidence interval, 0.792-0.947). Calibration plots and decision curve analysis showed good model performance in both datasets. A web-based calculator (https://bzxzmu.shinyapps.io/STEMI-with-Hyperuricemia-intrahospital-mortality/) was established based on the nomogram model, which was used to measure the levels of OHCA, neutrophil-to-lymphocyte ratio, shock index, α-HBDH, cystatin C, and B-type natriuretic peptides.
Conclusion: For practical applications, this model may prove clinically useful for personalized therapy management in patients with STEMI with hyperuricemia.
Keywords: STEMI; hyperuricemia; mortality; nomogram.
© 2021 Bai et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
