

Steroids and Olfactory Training for Postviral Olfactory Dysfunction: A Systematic Review
- PMID: 34456675
- PMCID: PMC8387929
- DOI: 10.3389/fnins.2021.708510
Steroids and Olfactory Training for Postviral Olfactory Dysfunction: A Systematic Review
Abstract
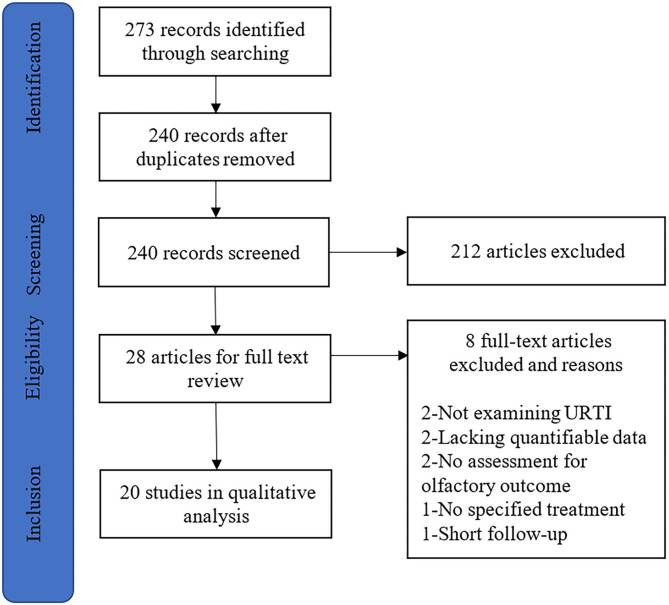
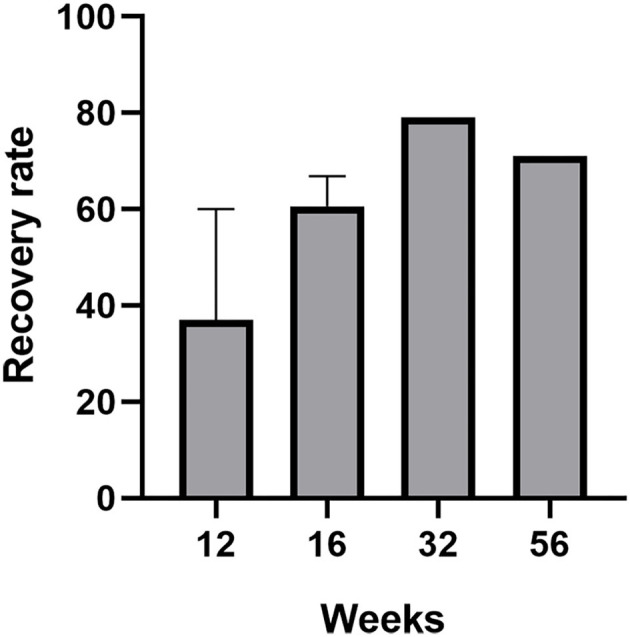
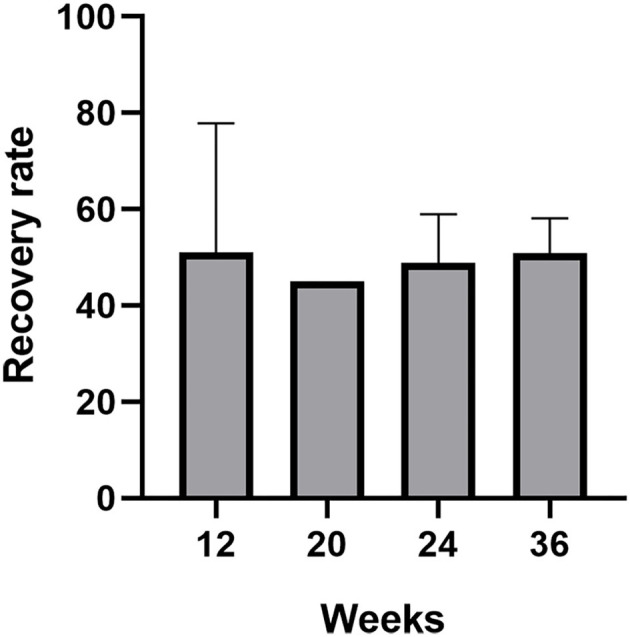
Background: Postviral olfactory dysfunction (PVOD) is a clinical challenge due to limited therapeutic options and poor prognosis. Both steroids and olfactory training have been proved to be effective for olfactory dysfunction with varied etiologies. We sought to perform a systematic review to summarize the evidence of steroids or olfactory training for patients with PVOD. Methods: A systematic literature review using PubMed, Embase, Cochrane Library, and Web of Science was conducted to identify studies assessing olfactory change in patients with PVOD receiving steroid or olfactory training. Results: Of the initial 273 abstracts reviewed, 20 articles with data from 2,415 patients with PVOD were included. Treatments including topical steroids, systemic steroids, classical olfactory training (COT), modified olfactory training (MOT), and olfactory training with steroid were analyzed. Both psychophysical olfactory testing and subjective symptom scores were utilized to assess the olfactory function. The routine use of nasal steroid spray alone during the management of PVOD seems to have no positive effect on olfactory dysfunction. Direct injection of steroid or nasal steroid spray into the olfactory cleft significantly improved the olfactory function in patients with PVOD. Olfactory improvement is greater than that of the natural course of the disease with short-term COT. Patients with PVOD would benefit more from long-term COT (>12 weeks). Treatment duration, various odorants, olfactory training devices, changing the types of odors periodically, different molecular odorants, and different concentrations of odorants tended to increase the efficiency of MOT. Clinically significant improvement after olfactory training was defined as an increase of threshold, discrimination, and identification (TDI) score ≥6. From week 24 to week 36, both COT and MOT groups reached the maximum therapeutic effect regarding the number of participants achieving clinically significant improvement. A combination of local or oral steroids with olfactory training is more efficient than COT only. Conclusion: Olfactory function in patients with PVOD was effectively improved through direct steroid administration in the olfactory cleft, COT, or modification of COT. The addition of topical steroids to COT therapy showed a tendency for greater olfactory improvement in patients with PVOD.
Keywords: olfactory dysfunction; olfactory training; postviral olfactory dysfunction; steroid; systematic review.
Copyright © 2021 Yuan, Huang, Wei and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Olfactory Training for Postviral Olfactory Dysfunction: Systematic Review and Meta-analysis.Otolaryngol Head Neck Surg. 2021 Feb;164(2):244-254. doi: 10.1177/0194599820943550. Epub 2020 Jul 14. Otolaryngol Head Neck Surg. 2021. PMID: 32660334
-
Treatment of post-viral olfactory dysfunction: an evidence-based review with recommendations.Int Forum Allergy Rhinol. 2020 Sep;10(9):1065-1086. doi: 10.1002/alr.22624. Epub 2020 Jun 25. Int Forum Allergy Rhinol. 2020. PMID: 32567798 Free PMC article.
-
Therapeutic Potential of Valproic Acid for Postviral Olfactory Dysfunction: A Single-Arm Pilot Study.Ann Otol Rhinol Laryngol. 2023 Jun;132(6):709-714. doi: 10.1177/00034894221111245. Epub 2022 Jul 13. Ann Otol Rhinol Laryngol. 2023. PMID: 35833237 Clinical Trial.
-
Therapeutic use of steroids in non-chronic rhinosinusitis olfactory dysfunction: a systematic evidence-based review with recommendations.Int Forum Allergy Rhinol. 2019 Feb;9(2):165-176. doi: 10.1002/alr.22240. Epub 2018 Nov 24. Int Forum Allergy Rhinol. 2019. PMID: 30472771
-
Is SARS-CoV-2 (COVID-19) postviral olfactory dysfunction (PVOD) different from other PVOD?World J Otorhinolaryngol Head Neck Surg. 2020 Nov;6(Suppl 1):S26-S32. doi: 10.1016/j.wjorl.2020.05.004. Epub 2020 May 19. World J Otorhinolaryngol Head Neck Surg. 2020. PMID: 32837756 Free PMC article. Review.
Cited by
-
Characterization of Ethyl Butyrate-Induced Cough Before and After Breath Control Techniques in Healthy Adults.Am J Speech Lang Pathol. 2023 Mar 9;32(2):675-687. doi: 10.1044/2022_AJSLP-22-00233. Epub 2023 Jan 12. Am J Speech Lang Pathol. 2023. PMID: 36634229 Free PMC article. Clinical Trial.
-
Effect of Olfactory Rehabilitation on the Recovery of Post-Coronavirus Disease Olfactory Dysfunction: A Randomized Controlled Trial.Cureus. 2024 Jun 6;16(6):e61855. doi: 10.7759/cureus.61855. eCollection 2024 Jun. Cureus. 2024. PMID: 38975544 Free PMC article.
-
Topical Administration of Mometasone Is Not Helpful in Post-COVID-19 Olfactory Dysfunction.Life (Basel). 2022 Sep 24;12(10):1483. doi: 10.3390/life12101483. Life (Basel). 2022. PMID: 36294918 Free PMC article.
-
Recovery of Smell and Taste in Patients With Persistent COVID-19-Related Hyposmia and Dysgeusia by Targeting Inflammation and Endothelial Dysfunction.Cureus. 2024 Feb 26;16(2):e54925. doi: 10.7759/cureus.54925. eCollection 2024 Feb. Cureus. 2024. PMID: 38544584 Free PMC article.
-
A multicenter real-life study to determine the efficacy of corticosteroids and olfactory training in improving persistent COVID-19-related olfactory dysfunction.Laryngoscope Investig Otolaryngol. 2022 Dec 2;8(1):46-54. doi: 10.1002/lio2.989. Online ahead of print. Laryngoscope Investig Otolaryngol. 2022. PMID: 36718474 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous