

Neurological Manifestations of Coronavirus Disease 2019: A Comprehensive Review and Meta-Analysis of the First 6 Months of Pandemic Reporting
- PMID: 34456840
- PMCID: PMC8387564
- DOI: 10.3389/fneur.2021.664599
Neurological Manifestations of Coronavirus Disease 2019: A Comprehensive Review and Meta-Analysis of the First 6 Months of Pandemic Reporting
Abstract
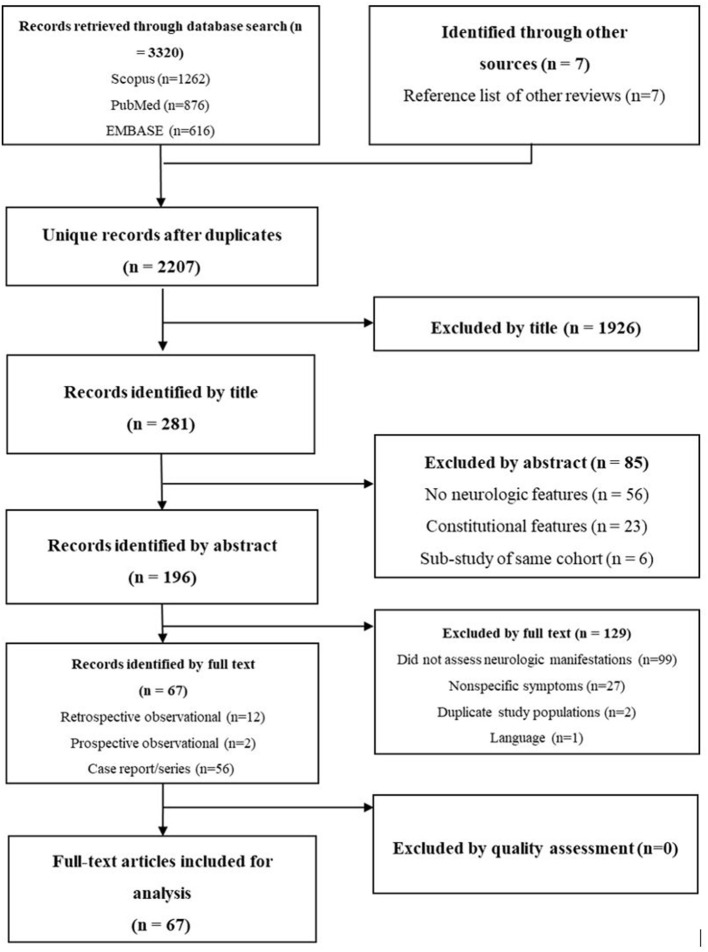
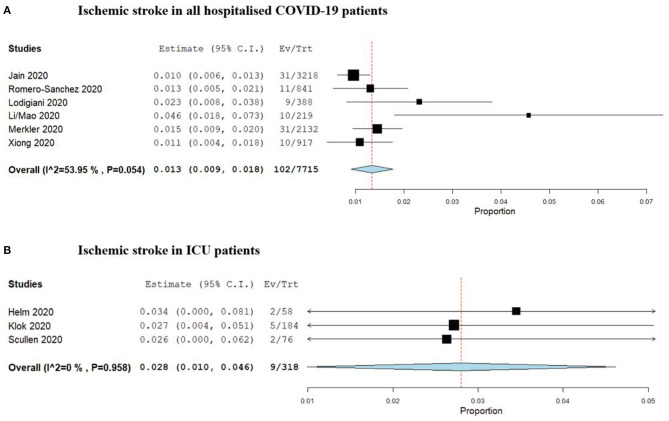
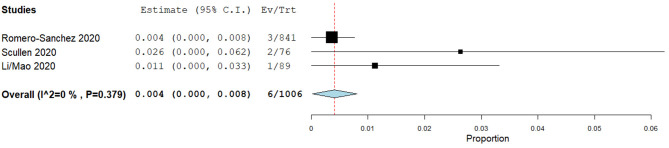
Background: There is growing evidence that SARS-Cov-2 infection is associated with severe neurological complications. Understanding the nature and prevalence of these neurologic manifestations is essential for identifying higher-risk patients and projecting demand for ongoing resource utilisation. This review and meta-analysis report the neurologic manifestations identified in hospitalised COVID-19 patients and provide a preliminary estimate of disease prevalence. Methods: MEDLINE, Embase and Scopus were searched for studies reporting the occurrence of neurological complications in hospitalised COVID-19 patients. Results: A total of 2,207 unique entries were identified and screened, among which 14 cohort studies and 53 case reports were included, reporting on a total of 8,577 patients. Central nervous system manifestations included ischemic stroke (n = 226), delirium (n = 79), intracranial haemorrhage (ICH, n = 57), meningoencephalitis (n = 13), seizures (n = 3), and acute demyelinating encephalitis (n = 2). Peripheral nervous system manifestations included Guillain-Barrè Syndrome (n = 21) and other peripheral neuropathies (n = 3). The pooled period prevalence of ischemic stroke from identified studies was 1.3% [95%CI: 0.9-1.8%, 102/7,715] in all hospitalised COVID-19 patients, and 2.8% [95%CI: 1.0-4.6%, 9/318] among COVID-19 patients admitted to ICU. The pooled prevalence of ICH was estimated at 0.4% [95%CI: 0-0.8%, 6/1,006]. Conclusions: The COVID-19 pandemic exerts a substantial neurologic burden which may have residual effects on patients and healthcare systems for years. Low quality evidence impedes the ability to accurately predict the magnitude of this burden. Robust studies with standardised screening and case definitions are required to improve understanding of this disease and optimise treatment of individuals at higher risk for neurologic sequelae.
Keywords: COVID-19; critical care; intensive care; neurological complication; neurological injury.
Copyright © 2021 Huth, Cho, Robba, Highton, Battaglini, Bellapart, Suen, Li Bassi, Taccone, Arora, Whitman, Fraser and Fanning.
Conflict of interest statement
The authors are all members of the COVID-19 Critical Care Consortium Neurology sub-committee. RA has received an unrestricted educational grant from Pfizer Canada Inc. and honoraria from Mallinckrodt Pharmaceutical, Abbott Nutrition and Edwards Lifesciences that are. GW received funding from the Data Safety Monitoring board of Cytosorbent and Cellphire. GLB receives grant support from University of Queensland, Wesley Medical Research, The Prince Charles Hospital Foundation, The Health Research Board of Ireland, Biomedicine International Training Research Program for Excellent Clinician-Scientists, European Union's Research and Innovation Program (Horizon 2020), and La Caixa Foundation. GLB and JFF have received research support from Fisher & Paykel. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous