

High Neutrophil-To-Lymphocyte Ratio Is an Independent Risk Factor for End Stage Renal Diseases in IgA Nephropathy
- PMID: 34456912
- PMCID: PMC8387559
- DOI: 10.3389/fimmu.2021.700224
High Neutrophil-To-Lymphocyte Ratio Is an Independent Risk Factor for End Stage Renal Diseases in IgA Nephropathy
Abstract
Background: Complex factors are involved in the development and progression of immunoglobulin A nephropathy (IgAN), a common primary glomerulonephritis worldwide. Autoimmunity and inflammation have been considered to be the basic mechanisms; however, the exact pathogenesis remains unclear. As a novel marker of inflammation, the neutrophil-to-lymphocyte ratio (NLR) has been studied in various diseases. Whether the NLR can predict the renal outcome of patients with IgAN remains unclear. We evaluated the relationships between the NLR and renal function, pathologic lesions, renal progression, and prognosis in patients with IgAN.
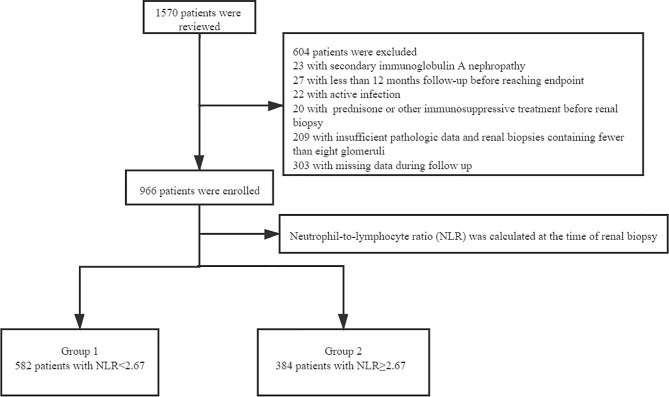
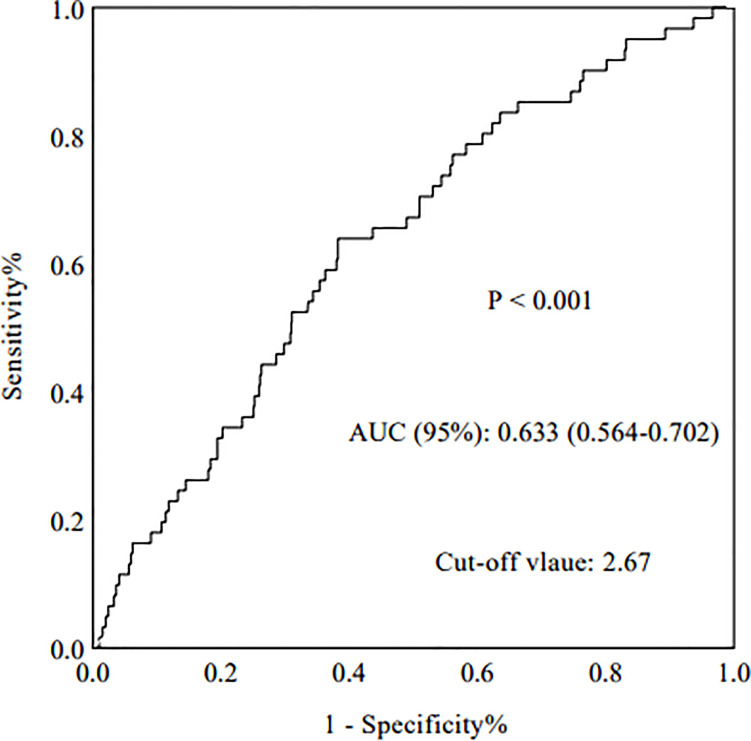
Methods: This retrospective study involved 966 patients with biopsy-proven IgAN. They were divided into two groups based on the cut-off value of the NLR: the high group (NLR ≥ 2.67, n = 384) and the low group (NLR < 2.67, n = 582). The endpoint was end-stage renal disease [estimated glomerular filtration rate (eGFR) of <15 mL/min/1.73 m2 or performance of renal replacement therapy]. A correlation test was conducted to explore the relationship between the NLR and other important parameters (eGFR, serum creatinine, proteinuria, hypertension and renal pathologic lesions). The predictive value was determined by the area under the receiver operating characteristics curve (AUROC). Kaplan-Meier and Cox proportional hazards analyses were performed to evaluate renal progression and prognosis.
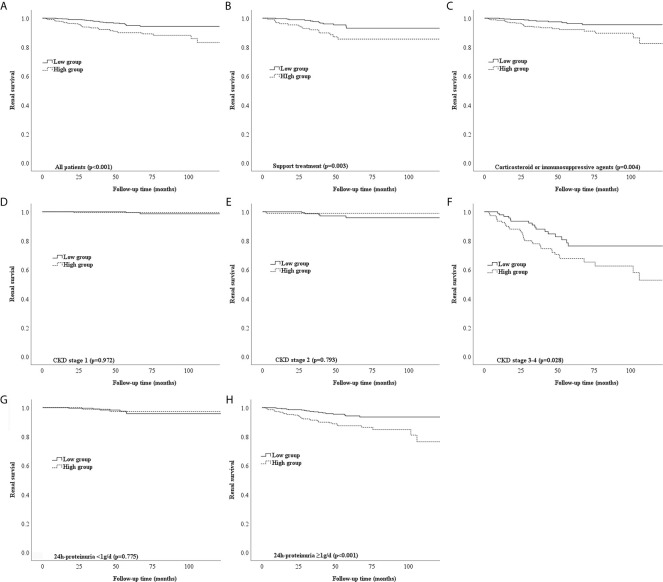
Results: The NLR had the highest AUROC, which was 0.633 (p < 0.001). The correlation test revealed that the NLR was positively correlated with serum creatinine (r = 0.127, p < 0.001) and 24-hour urine protein (r = 0.18, p < 0.001) and negatively correlated with eGFR (r = 0.14, p < 0.001). Patients with IgAN who had a high NLR were more likely to have hypertension (p = 0.003). Multivariate Cox regression analysis indicated that a high NLR was an independent risk factor for IgAN even after adjustment for important clinical and pathological parameters (p = 0.043, HR = 1.74, 95%CI: 1.02-2.97). Kaplan-Meier analysis showed that a high NLR was significantly associated with the renal prognosis of patients with IgAN (p < 0.001), especially patients with stage 3 to 4 chronic kidney disease (p = 0.028) or 24-hour urine protein of >1 g/day (p < 0.001).
Conclusion: An elevated NLR affects the renal progression and prognosis in patients with IgAN and could be a marker for evaluation of renal function and pathologic lesions.
Keywords: IgA nephropathy; neutrophil-to-lymphocyte ratio (NLR); pathologic lesions; renal prognosis; renal progression.
Copyright © 2021 Wang, Dong, Pei, Jiang, Qin, Tan, Tang and Qin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Relationship between blood neutrophil-lymphocyte ratio and renal tubular atrophy/interstitial fibrosis in IgA nephropathy patients.J Clin Lab Anal. 2021 Jun;35(6):e23774. doi: 10.1002/jcla.23774. Epub 2021 May 5. J Clin Lab Anal. 2021. PMID: 33951240 Free PMC article.
-
Prognostic nutritional index as an independent risk factor for disease progression in patients with IgA nephropathy.Front Med (Lausanne). 2025 Feb 25;12:1530312. doi: 10.3389/fmed.2025.1530312. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40070651 Free PMC article.
-
The prognostic value of the systemic immune inflammation index in patients with IgA nephropathy.Ren Fail. 2024 Dec;46(2):2381613. doi: 10.1080/0886022X.2024.2381613. Epub 2024 Jul 22. Ren Fail. 2024. PMID: 39039867 Free PMC article.
-
Immunoglobulin a nephropathy: Pathological markers of renal survival in paediatric patients.Nephrology (Carlton). 2016 Dec;21(12):995-1002. doi: 10.1111/nep.12850. Nephrology (Carlton). 2016. PMID: 27414046 Review.
-
Markers for the progression of IgA nephropathy.J Nephrol. 2016 Aug;29(4):535-41. doi: 10.1007/s40620-016-0299-0. Epub 2016 May 3. J Nephrol. 2016. PMID: 27142988 Free PMC article. Review.
Cited by
-
The association between type 1 diabetes mellitus and the risk of immunoglobulin A nephropathy: a Mendelian randomization study.Front Med (Lausanne). 2024 Dec 18;11:1429369. doi: 10.3389/fmed.2024.1429369. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39744534 Free PMC article.
-
The association of neutrophil-to-lymphocyte ratio with post-chemotherapy pulmonary infection in lung cancer patients.Front Med (Lausanne). 2025 Apr 9;12:1559702. doi: 10.3389/fmed.2025.1559702. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40270508 Free PMC article.
-
Is hyperuricemia an independent prognostic factor for IgA nephropathy: a systematic review and meta-analysis of observational cohort studies.Ren Fail. 2022 Dec;44(1):70-80. doi: 10.1080/0886022X.2021.2019589. Ren Fail. 2022. PMID: 35156903 Free PMC article.
-
Uric acid-based ratios for predicting renal failure in Chinese IgA nephropathy patients.Int J Med Sci. 2023 Sep 25;20(12):1584-1591. doi: 10.7150/ijms.85430. eCollection 2023. Int J Med Sci. 2023. PMID: 37859692 Free PMC article.
-
Neutrophil-Lymphocyte, Platelet-Neutrophil, and Platelet-Lymphocyte Ratios as Indicators of Sickle Cell Anaemia Severity.Ethiop J Health Sci. 2023 Sep;33(5):821-830. doi: 10.4314/ejhs.v33i5.12. Ethiop J Health Sci. 2023. PMID: 38784518 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous