

Apoptotic Gastritis in Melanoma Patients Treated With PD-1-Based Immune Checkpoint Inhibition - Clinical and Histopathological Findings Including the Diagnostic Value of Anti-Caspase-3 Immunohistochemistry
- PMID: 34458154
- PMCID: PMC8385713
- DOI: 10.3389/fonc.2021.725549
Apoptotic Gastritis in Melanoma Patients Treated With PD-1-Based Immune Checkpoint Inhibition - Clinical and Histopathological Findings Including the Diagnostic Value of Anti-Caspase-3 Immunohistochemistry
Abstract
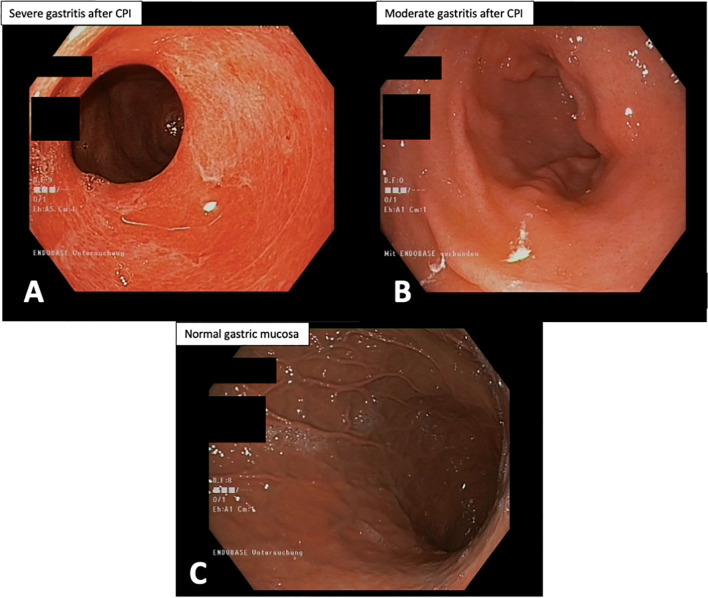
Background: Gastritis induced by checkpoint inhibitors (CPI) is a rare but severe drug-related side effect. The reference standard for confirming CPI-associated gastritis (CPI-assGastritis) is histopathological assessment; however, the histopathological features of CPI-assGastritis are not yet adequately defined.
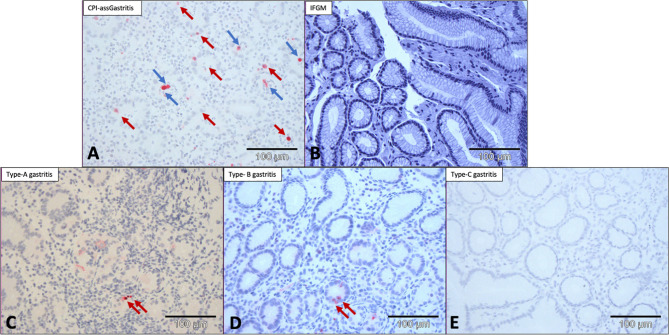
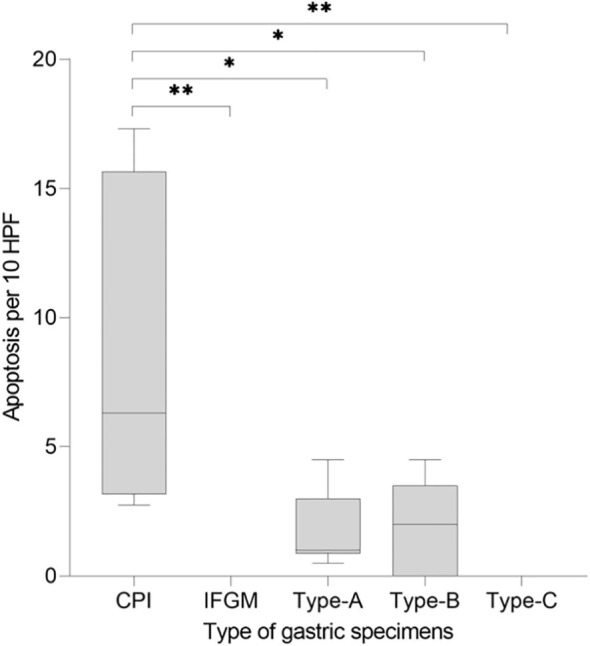
Materials and methods: Gastric biopsies of melanoma patients with histopathologically suspected CPI-assGastritis were compared with gastric biopsies of patients with inflammation free gastric mucosa (IFGM), type A, B, and C gastritis with respect to apoptosis count and predominant histopathological features. Immunohistochemical anti-caspase-3 staining was performed to identify apoptosis. Quantification was performed by manually counting the number of apoptotic events per 10 high-power fields (HPF). Clinical symptoms, treatment, and follow-up data of patients with CPI-assGastritis were examined. The nonparametric Mann-Whitney U test was used for statistical testing.
Results: Five melanoma patients (three women, two men; median age: 45 years) were treated with PD-1-based CPI. The patients reported epigastric pain, weight loss, nausea, and vomiting. Histologically, the patients with CPI-assGastritis showed a partly lymphocytic, partly granulocytic inflammatory infiltrate. Manual counting of apoptotic cells in biopsy tissue slides stained against caspase 3 revealed a median of 6 apoptotic events/10 HPF (95% CI, 2.75-17.30) in the patients with CPI-assGastritis. Results for the comparison cohort (patients n = 21) were a median of 1 apoptotic event/10 HPF (95% CI, 0.5-4.5) for type-A gastritis (six patients), a median of 2 apoptotic events/10 HPF (95% CI, 0-4.5) for type-B gastritis (five patients), and no apoptosis for IFGM and type-C gastritis (five patients). Patients with CPI-assGastritis had a significantly higher apoptosis count than patients with IFGM (p<0.01), type A (p<0.05), B (p<0.05), and C gastritis (p<0.01). None of the CPI-assGastritis biopsies showed evidence of Helicobacter pylori. All CPI-assGastritis patients responded to systemic treatment with corticosteroids.
Conclusion: CPI-assGastritis manifests with nonspecific symptoms but histologically shows a high number of apoptotic events, which can best be visualized by anti-caspase-3 immunohistochemistry. This histopathological feature may help to histologically differentiate CPI-assGastritis from other forms of gastritis and inform decision-making regarding its optimal management.
Keywords: PD-1; gastritis; immune check inhibitor (ICI); immune related adverse effects; melanoma.
Copyright © 2021 Placke, Rawitzer, Reis, Rashidi-Alavijeh, Livingstone, Ugurel, Hadaschik, Griewank, Schmid, Schadendorf, Roesch and Zimmer.
Conflict of interest statement
J-MP served as consultant and/or has received honoraria from Bristol-Myers Squibb and Novartis, and has received travel support from Bristol-Myers Squibb, Novartis and Therakos. HR is on the advisory board of Bristol-Myers Squibb, received honoraria from Roche and Bristol-Myers Squibb, received travel support from Philips, Roche, and Bristol-Myers Squibb, received grants from Bristol-Myers Squibb and holds shares of Bayer. EL served as consultant or/and has received honoraria from Amgen, Actelion, Roche, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Janssen, Medac, Sanofi, and Sunpharma, and travel support from Amgen, Merck Sharp & Dohme, Bristol-Myers Squibb, Amgen, Pierre-Fabre, Sunpharma, and Novartis, outside the submitted work. SU received grants, personal fees, and non-financial support from Novartis, grants and non-financial support from Bristol-Myers Squibb; personal fees and non-financial support from Roche, personal fees from Merck Sharp & Dohme, and non-financial support from Amgen, outside the submitted work. DS received grants and other support from Bristol-Myers Squibb, personal fees from Bristol-Myers Squibb during the conduct of the study, personal fees from Amgen, personal fees from Boehringer Ingelheim, personal fees from InFlarX, personal fees and other support from Roche, grants, personal fees and other support from Novartis, personal fees from Incyte, personal fees and other support from Regeneron, personal fees from 4SC, personal fees from Sanofi, personal fees from Neracare, personal fees from Pierre-Fabre, personal fees and other support from Merck-EMD, personal fees from Pfizer, personal fees and other support from Philogen, personal fees from Array, personal fees and other support from MSD Sharp & Dohme, outside the submitted work. AR reported grants from Novartis, Bristol Myers Squibb, and Adtec, personal fees from Merck Sharp & Dohme, and nonfinancial support from Amgen, Roche, Merck Sharp & Dohme, Novartis, Bristol Myers Squibb, and Teva. LZ served as consultant and/or has received honoraria from Roche, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre-Fabre, and Sanofi, research funding to institution from Novartis, travel support from Merck Sharp & Dohme, Bristol-Myers Squibb, Amgen, Pierre-Fabre, and Novartis, outside the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
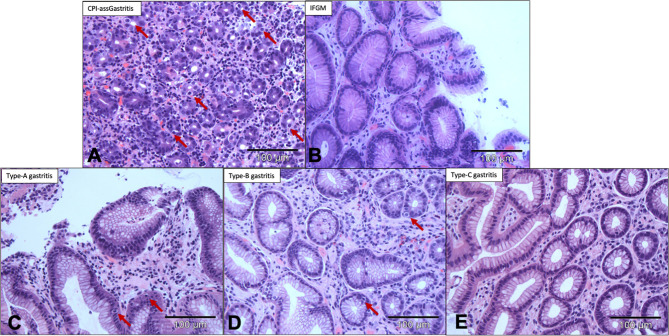
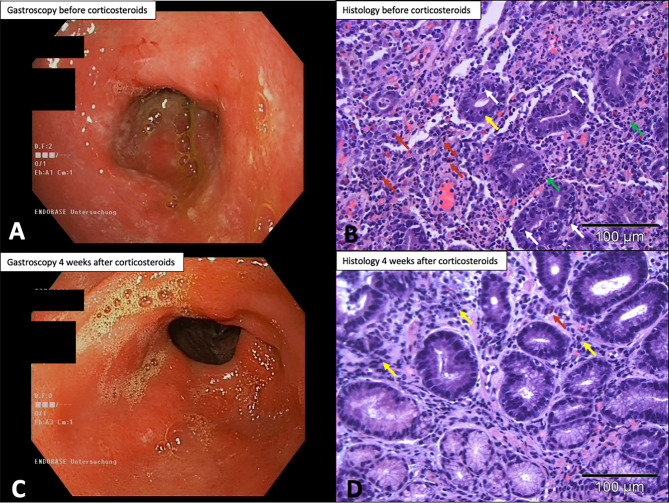
 , apoptosis;
, apoptosis;  , eosinophilic granulocytes;
, eosinophilic granulocytes;  , neutrophilic granuolocytes;
, neutrophilic granuolocytes;  , lymphocytes.
, lymphocytes.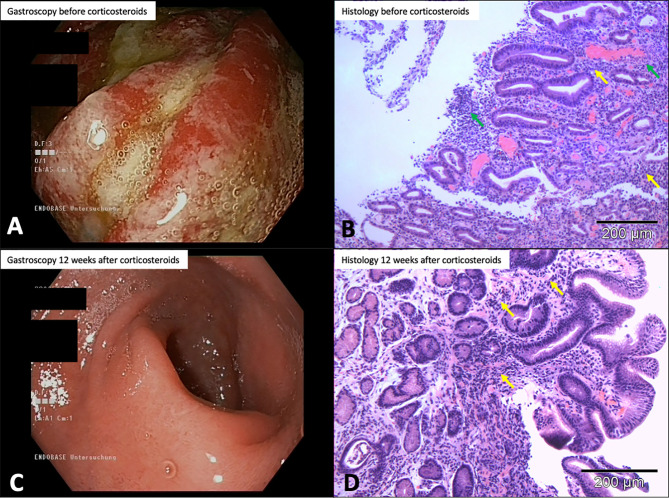
References
-
- Kaufman HL, Russell J, Hamid O, Bhatia S, Terheyden P, D’Angelo SP, et al. . Avelumab in Patients With Chemotherapy-Refractory Metastatic Merkel Cell Carcinoma: A Multicentre, Single-Group, Open-Label, Phase 2 Trial. Lancet Oncol (2016) 17(10):1374–85. 10.1016/S1470-2045(16)30364-3 - DOI - PMC - PubMed
-
- Motzer RJ, Rini BI, McDermott DF, Arén Frontera O, Hammers HJ, Carducci MA, et al. . Nivolumab Plus Ipilimumab Versus Sunitinib in First-Line Treatment for Advanced Renal Cell Carcinoma: Extended Follow-Up of Efficacy and Safety Results From a Randomised, Controlled, Phase 3 Trial. Lancet Oncol (2019) 20(10):1370–85. 10.1016/S1470-2045(19)30413-9 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials