

Myoglobin Offers Higher Accuracy Than Other Cardiac-Specific Biomarkers for the Prognosis of COVID-19
- PMID: 34458331
- PMCID: PMC8387634
- DOI: 10.3389/fcvm.2021.686328
Myoglobin Offers Higher Accuracy Than Other Cardiac-Specific Biomarkers for the Prognosis of COVID-19
Abstract
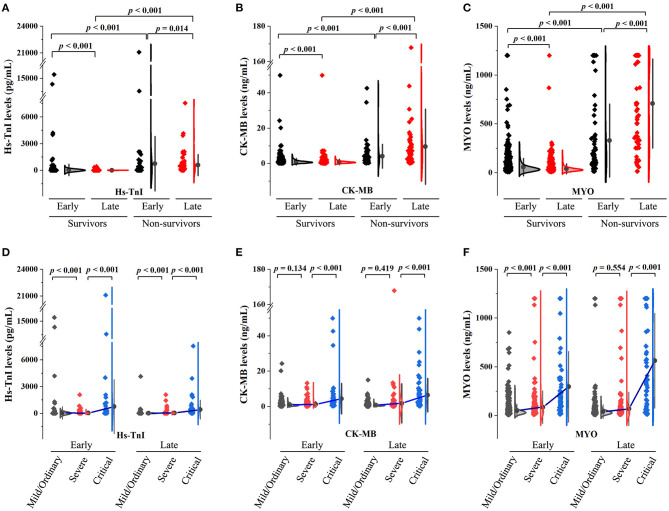
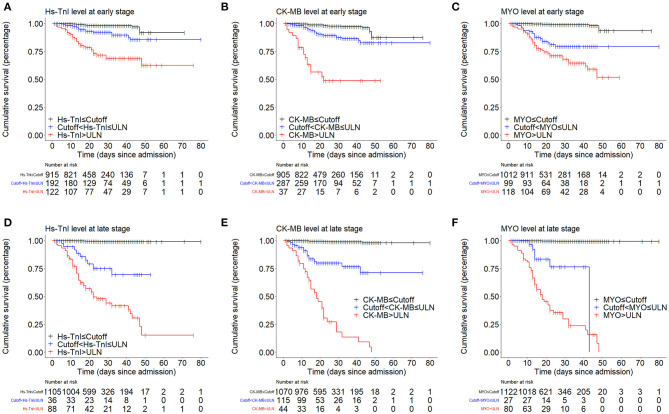
Although sporadic studies have shown that myoglobin may have better prognostic performance than other cardiac markers in COVID-19, a comprehensive comparative study is lacking. Herein, we retrospectively analyzed the clinical and laboratory data of COVID-19 patients admitted to the Guanggu Campus of Wuhan Tongji Hospital from February 9, 2020 to March 30, 2020, intending to compare the prognostic accuracy of three commonly used cardiac markers on COVID-19 mortality. Our results revealed that abnormal increases in myocardial biomarkers were associated with a significantly increased risk of in-hospital mortality with COVID-19. Interestingly, myoglobin, a non-cardiac-specific biomarker, also expressed in skeletal myocytes, had even higher prognostic accuracy than cardiac-specific biomarkers such as high-sensitivity troponin I (hs-TnI) and creatine kinase-MB (CK-MB). More importantly, multivariate Cox analysis showed that myoglobin, rather than hs-TnI or CK-MB, was independently prognostic for in-hospital mortality in COVID-19. These results were further confirmed by subgroup analyses of patients with severe and critical illnesses and those without a history of cardiovascular disease. Our findings suggest that myoglobin may be a reliable marker of illness reflecting general physiological disturbance and help to assess prognosis and treatment response in patients with COVID-19.
Keywords: COVID-19; in-hospital mortality; myocardial biomarkers; myoglobin; rhabdomyolysis.
Copyright © 2021 Yu, Chen, Zeng, Yang and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous