

Natural antibody and complement activation characterize patients with idiopathic nephrotic syndrome
- PMID: 34459222
- PMCID: PMC8560405
- DOI: 10.1152/ajprenal.00041.2021
Natural antibody and complement activation characterize patients with idiopathic nephrotic syndrome
Abstract
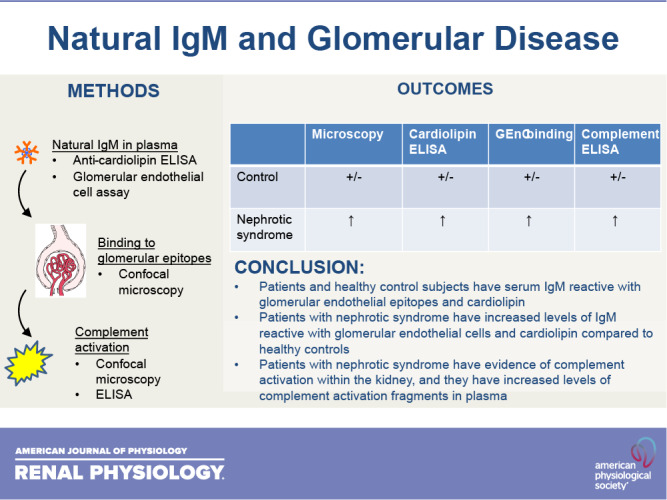
Focal segmental glomerulosclerosis (FSGS) and minimal change disease (MCD) are common forms of idiopathic nephrotic syndrome. The causes of these diseases are incompletely understood, but the response of patients to immunosuppressive therapies suggests that their pathogenesis is at least in part immune mediated. Preclinical and clinical research indicates that activation of the classical pathway of complement contributes to glomerular injury in FSGS. Glomerular IgM deposits are also prominent in some patients, raising the possibility that IgM is a trigger of classical pathway activation. In the present study, we examined the pattern of complement activation in the glomeruli and plasma of patients with nephrotic syndrome. We also tested whether patients with FSGS and MCD have elevated levels of natural IgM reactive with epitopes on glomerular endothelial cells and cardiolipin. We found evidence of classical pathway activation in patients with idiopathic nephrotic syndrome compared with healthy control subjects. We also detected higher levels of self-reactive IgM to both targets. Based on these results, IgM and classical pathway activation may contribute to disease pathogenesis in some patients with FSGS and MCD.NEW & NOTEWORTHY IgM is detected in biopsies from some patients with nephrotic syndrome, although this has been attributed to passive trapping of the protein. We found, however, that IgM colocalizes with complement activation fragments in some glomeruli. We also found that affected patients had higher levels of IgM reactive to glomerular endothelial cell epitopes. Thus, IgM activates the complement system in the glomeruli of some patients with nephrotic syndrome and may contribute to injury.
Keywords: IgM; complement; focal segmental glomerulosclerosis; minimal change disease; nephrotic syndrome.
Conflict of interest statement
J.M.T. and V.M.H. receive royalties from Alexion Pharmaceuticals, Inc., and are consultants for Q32 Bio, Inc., a company developing complement inhibitors. They also hold stock and will receive royalty income from Q32 Bio, Inc. S.L.K. and F.L. are employed by Q32 Bio, Inc. H.T. is a consultant to Otsuka (Chair, DSMB) and Chemocentryx (DSMB). He has consultancy agreements through NYU Grossman School of Medicine with Retrophin Inc. and Goldfinch Bio Inc. None of the other authors has any conflicts of interest, financial or otherwise, to disclose.
Figures







References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- DK076690/HHS | NIH | National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
- K23 DK122136/DK/NIDDK NIH HHS/United States
- DK113586/HHS | NIH | National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
- U54 DK083912/DK/NIDDK NIH HHS/United States
- R01 DK113586/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases