

Sodium-Glucose Co-Transporter Inhibitors and Atrial Fibrillation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 34459238
- PMCID: PMC8649253
- DOI: 10.1161/JAHA.121.022222
Sodium-Glucose Co-Transporter Inhibitors and Atrial Fibrillation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
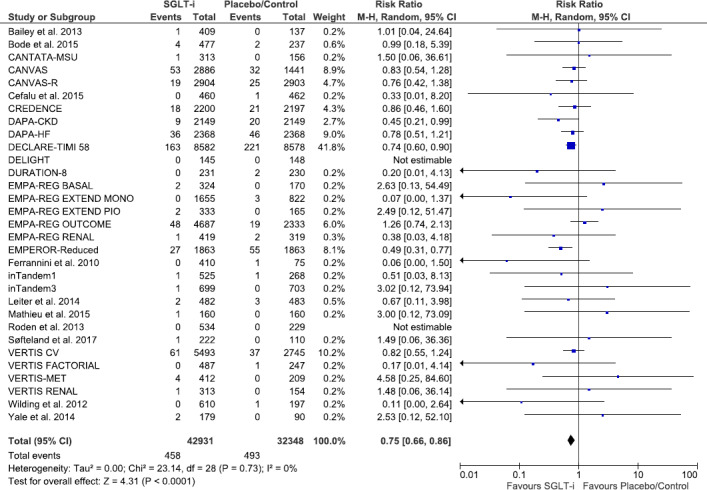
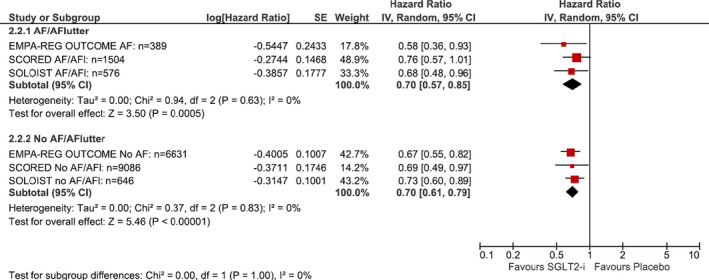
Background Sodium-glucose co-transporter (SGLT) inhibitors reduce cardiovascular outcomes including mortality in several populations; however, their effect on atrial fibrillation/flutter (AF) remains unclear. Our objective was to determine whether SGLT inhibitors reduce AF and whether a history of AF modifies the effect of SGLT inhibitors on the composite of heart failure hospitalization or cardiovascular death. Methods and Results We searched MEDLINE, Embase, and CENTRAL to March 2021. Pairs of reviewers identified randomized controlled trials that compared an SGLT inhibitor with placebo or no therapy. We pooled data using RevMan 5.4.1, assessed risk of bias using the Cochrane tool, and determined the overall quality of evidence using Grades of Recommendation, Assessment, Development and Evaluation. Thirty-one eligible trials reported on AF events (75 279 participants, mean age 62 years, 35.0% women). Moderate quality evidence supported a lower risk of serious AF events with SGLT inhibitors (1.1% versus 1.5%; risk ratio 0.75 [95% CI, 0.66-0.86]; I2=0%). A similar reduction in total AF events was also noted with SGLT inhibitors. Three trials reported on heart failure hospitalization/cardiovascular death stratified by a baseline history of AF (18 832 participants, mean age 66 years, 38.1% women); in patients with a history of AF, SGLT inhibitors resulted in a lower risk in the composite of heart failure hospitalization or cardiovascular death (hazard ratio, 0.70 [95% CI, 0.57-0.85]; I2=0%)-similar to the effect estimate for patients without AF, P value for interaction: 1.00. Conclusions SGLT inhibitors may reduce AF events and likely reduce heart failure hospitalization/cardiovascular death to a similar extent in patients with and without AF.
Keywords: SGLT inhibitors; atrial fibrillation; atrial flutter; gliflozins.
Conflict of interest statement
Dr Belley‐Cote reports grants from Bayer and grants from Roche, outside the submitted work. Dr Conen reports consulting fees from Roche Diagnostics outside of the current work. Dr Verma reports grants from Amarin, grants and personal fees from Amgen, grants and personal fees from AstraZeneca, grants and personal fees from Bayer, grants and personal fees from Boehringer‐Ingelheim, personal fees from Bristol‐Myers Squibb, grants and personal fees from Eli Lilly, personal fees from EOCI Pharmacomm Ltd, grants and personal fees from HLS Therapeutics, grants and personal fees from Janssen, grants and personal fees from Merck, personal fees from Novartis, grants and personal fees from Novo Nordisk, grants from Pfizer, grants from PhaseBio, grants and personal fees from Sanofi, personal fees from Sun Pharmaceuticals, personal fees from Toronto Knowledge Translation Working Group, outside the submitted work. Dr Gerstein reports grants and personal fees from Sanofi, grants and personal fees from Eli Lilly, grants and personal fees from Novo Nordisk, grants from AstraZeneca, grants from Merck, personal fees from Abbott, personal fees from Pfizer, personal fees from Boehringer Ingelheim, personal fees from DKSH, personal fees from Zuellig, sitting on a Data Safety Monitoring Board for Covance and sitting on a Data Safety Monitoring Board for Kowa, outside the submitted work. The remaining authors have no disclosures to report.
Figures
References
-
- Dorian P, Angaran P. Beta‐blockers and atrial fibrillation: hypertension and other medical conditions influencing their use. Can J Cardiol. 2014;30:S38–S41. - PubMed
-
- Gorenek B, Pelliccia A, Benjamin EJ, Boriani G, Crijns HJ, Fogel RI, Van Gelder IC, Halle M, Kudaiberdieva G, Lane DA, et al. European Heart Rhythm Association (EHRA)/European Association of Cardiovascular Prevention and Rehabilitation (EACPR) position paper on how to prevent atrial fibrillation endorsed by the Heart Rhythm Society (HRS) and Asia Pacific Heart Rhythm Society (APHRS). Eur J Prev Cardiol. 2017;24:4–40. DOI: 10.1177/2047487316676037. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
