

Evaluation of Gender Inequity in Thyroid Cancer Diagnosis: Differences by Sex in US Thyroid Cancer Incidence Compared With a Meta-analysis of Subclinical Thyroid Cancer Rates at Autopsy
- PMID: 34459841
- PMCID: PMC8406211
- DOI: 10.1001/jamainternmed.2021.4804
Evaluation of Gender Inequity in Thyroid Cancer Diagnosis: Differences by Sex in US Thyroid Cancer Incidence Compared With a Meta-analysis of Subclinical Thyroid Cancer Rates at Autopsy
Abstract
Importance: Thyroid cancer is more common in women than in men, but the associated causes of these differences are not fully understood.
Objective: To compare sex-specific thyroid cancer rates in the US to the prevalence of subclinical thyroid cancer at autopsy.
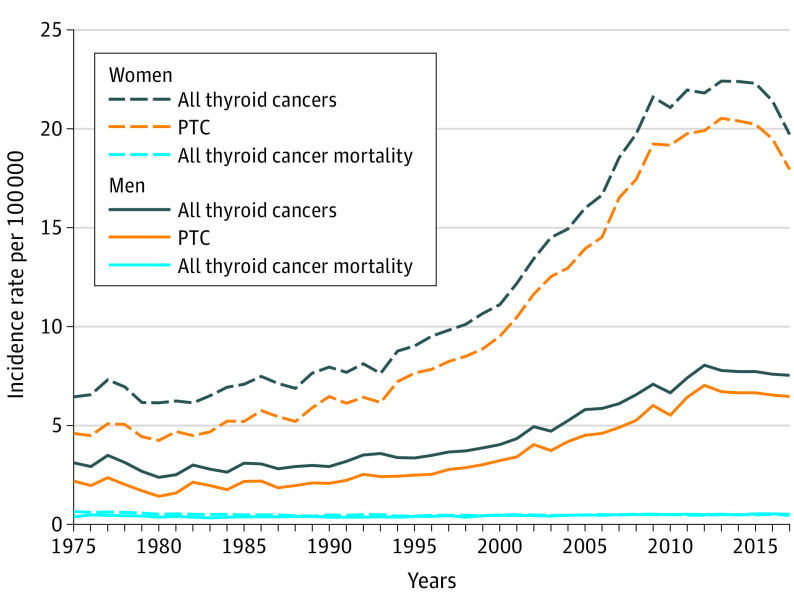
Data sources: Data on thyroid cancer incidence and mortality by sex among US adults (≥18 years) were extracted from the National Cancer Institute's Surveillance, Epidemiology, and End Results Program (SEER) data for 1975 to 2017. Embase, PubMed, and Web of Science databases were searched for studies on the prevalence of subclinical thyroid cancer at autopsy of men and women, from inception to May 31, 2021.
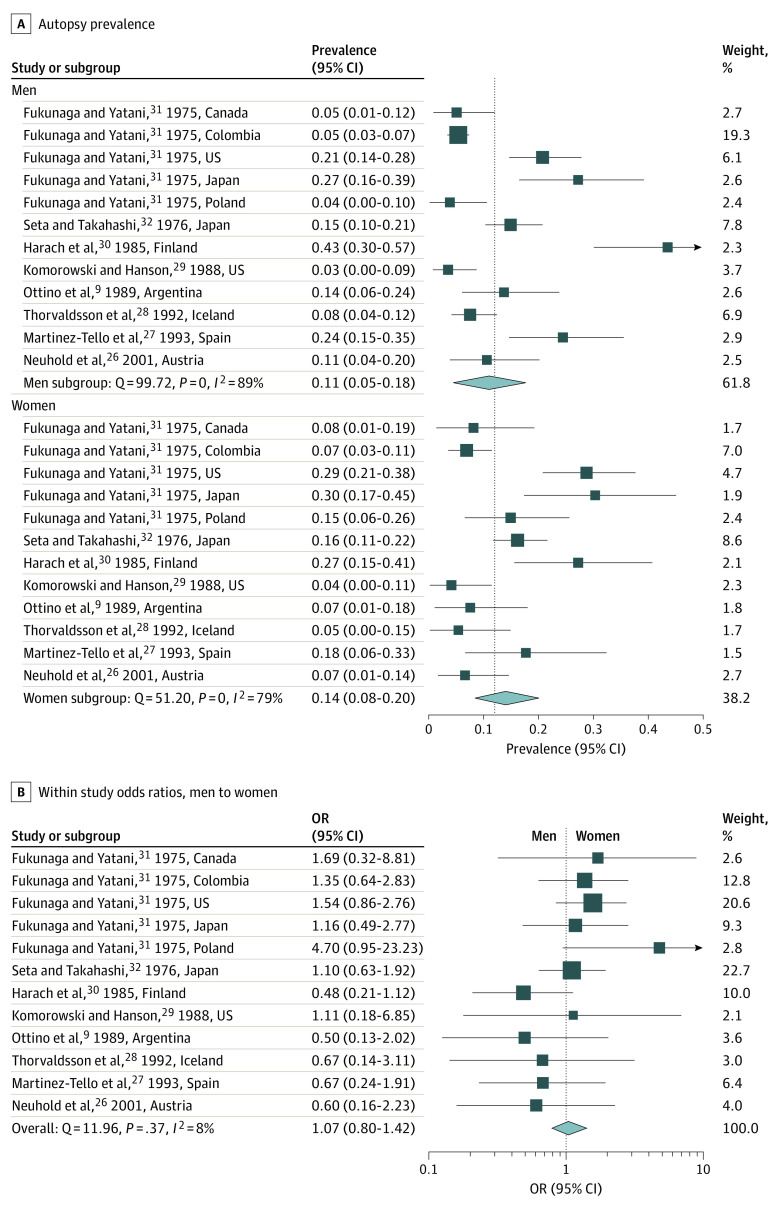
Study selection: The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline was used to perform a systematic search for articles reporting the prevalence of subclinical thyroid cancer in autopsy results of both women and men. Of 101 studies identified, 8 studies containing 12 data sets met inclusion criteria; ie, they examined the whole thyroid gland, stated the number of thyroids examined, and reported results by sex. Excluded studies reported thyroid cancer in Japan after the atomic bombs or Chernobyl after the nuclear disaster; did not examine the whole thyroid gland or had incomplete information on thyroid examination methods; or did not report rates by sex.
Data extraction and synthesis: Thyroid cancer incidence and mortality data by sex, histologic type, and tumor size were extracted from SEER. The inverse variance heterogeneity model was used to meta-analyze the prevalence and the odds ratio of subclinical thyroid cancer by sex from 8 studies (12 data sets) on thyroid cancer prevalence in autopsy results.
Main outcomes and measures: Incidence and mortality of thyroid cancer, by histologic type and tumor size; prevalence of thyroid cancer in autopsy results.
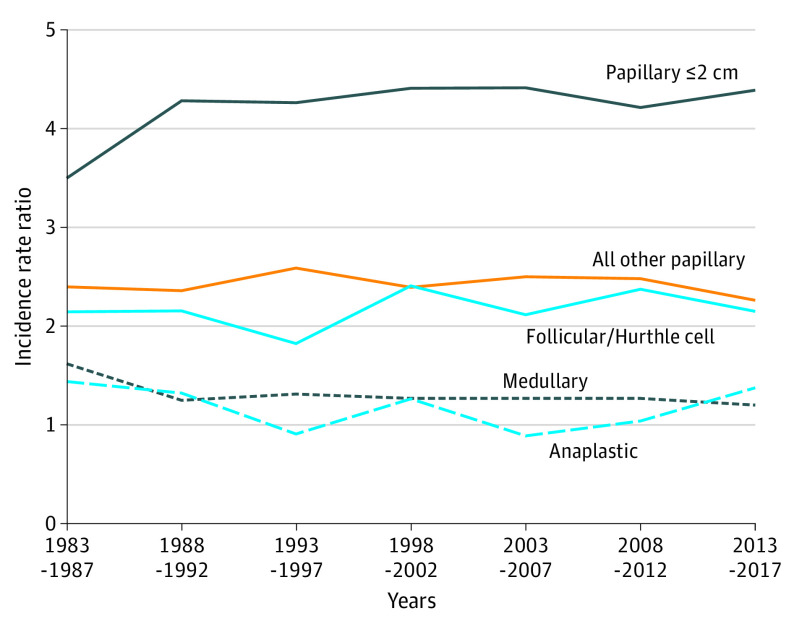
Results: In 2017, 90% of thyroid cancers diagnosed were papillary thyroid cancer (PTC) and in 2013 to 2017, the women to men incidence ratio for small (≤2 cm) PTC was 4.39:1. The incidence ratio approached 1:1 as cancer type lethality increased. The ratio of thyroid cancer mortality by gender was 1.02:1 and remained stable from 1992 to 2017. Results of the meta-analysis showed that the pooled autopsy prevalence of subclinical PTC was 14% in women (95% CI, 8%-20%) and 11% in men (95% CI, 5%-18%). The pooled odds ratio of subclinical PTC in women compared with men was 1.07 (95% CI, 0.80-1.42).
Conclusions and relevance: This cohort study and meta-analysis found that the belief that women get thyroid cancer more often than men is an oversimplification. The gender disparity is mostly confined to the detection of small subclinical PTCs, which are equally common in both sexes at autopsy but identified during life much more often in women than men. As the lethality of the cancer type increases, the ratio of detection by gender approaches 1:1. This phenomenon may be associated with gender differences in health care utilization and patterns of clinical thinking and can harm both women, who are subject to overdetection, and men, who may be at risk of underdetection.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
