

Risk of Rupture After Intracranial Aneurysm Growth
- PMID: 34459846
- PMCID: PMC8406207
- DOI: 10.1001/jamaneurol.2021.2915
Risk of Rupture After Intracranial Aneurysm Growth
Erratum in
-
Error in Figure.JAMA Neurol. 2022 Mar 1;79(3):312. doi: 10.1001/jamaneurol.2021.5146. JAMA Neurol. 2022. PMID: 35006239 Free PMC article. No abstract available.
Abstract
Importance: Unruptured intracranial aneurysms not undergoing preventive endovascular or neurosurgical treatment are often monitored radiologically to detect aneurysm growth, which is associated with an increase in risk of rupture. However, the absolute risk of aneurysm rupture after detection of growth remains unclear.
Objective: To determine the absolute risk of rupture of an aneurysm after detection of growth during follow-up and to develop a prediction model for rupture.
Design, setting, and participants: Individual patient data were obtained from 15 international cohorts. Patients 18 years and older who had follow-up imaging for at least 1 untreated unruptured intracranial aneurysm with growth detected at follow-up imaging and with 1 day or longer of follow-up after growth were included. Fusiform or arteriovenous malformation-related aneurysms were excluded. Of the 5166 eligible patients who had follow-up imaging for intracranial aneurysms, 4827 were excluded because no aneurysm growth was detected, and 27 were excluded because they had less than 1 day follow-up after detection of growth.
Exposures: All included aneurysms had growth, defined as 1 mm or greater increase in 1 direction at follow-up imaging.
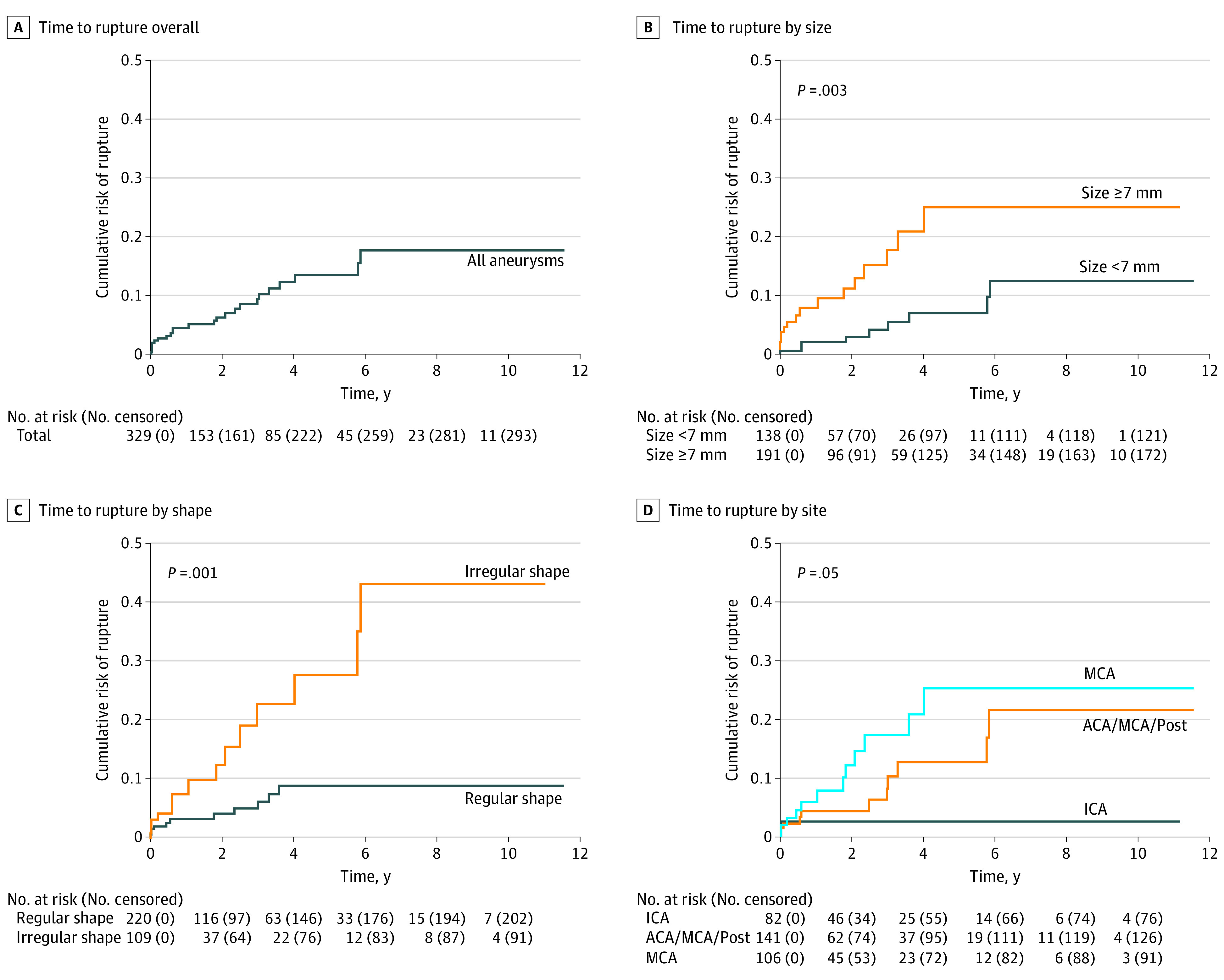
Main outcomes and measures: The primary outcome was aneurysm rupture. The absolute risk of rupture was measured with the Kaplan-Meier estimate at 3 time points (6 months, 1 year, and 2 years) after initial growth. Cox proportional hazards regression was used to identify predictors of rupture after growth detection.
Results: A total of 312 patients were included (223 [71%] were women; mean [SD] age, 61 [12] years) with 329 aneurysms with growth. During 864 aneurysm-years of follow-up, 25 (7.6%) of these aneurysms ruptured. The absolute risk of rupture after growth was 2.9% (95% CI, 0.9-4.9) at 6 months, 4.3% (95% CI, 1.9-6.7) at 1 year, and 6.0% (95% CI, 2.9-9.1) at 2 years. In multivariable analyses, predictors of rupture were size (7 mm or larger hazard ratio, 3.1; 95% CI, 1.4-7.2), shape (irregular hazard ratio, 2.9; 95% CI, 1.3-6.5), and site (middle cerebral artery hazard ratio, 3.6; 95% CI, 0.8-16.3; anterior cerebral artery, posterior communicating artery, or posterior circulation hazard ratio, 2.8; 95% CI, 0.6-13.0). In the triple-S (size, site, shape) prediction model, the 1-year risk of rupture ranged from 2.1% to 10.6%.
Conclusion and relevance: Within 1 year after growth detection, rupture occurred in approximately 1 of 25 aneurysms. The triple-S risk prediction model can be used to estimate absolute risk of rupture for the initial period after detection of growth.
Conflict of interest statement
Figures
References
-
- Algra AM, Lindgren A, Vergouwen MDI, et al. Procedural clinical complications, case-fatality risks, and risk factors in endovascular and neurosurgical treatment of unruptured intracranial aneurysms: a systematic review and meta-analysis. JAMA Neurol. 2019;76(3):282-293. doi: 10.1001/jamaneurol.2018.4165 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
