

Peritumoral edema status of glioblastoma identifies patients reaching long-term disease control with specific progression patterns after tumor resection and high-dose proton boost
- PMID: 34459971
- PMCID: PMC8557163
- DOI: 10.1007/s00432-021-03765-6
Peritumoral edema status of glioblastoma identifies patients reaching long-term disease control with specific progression patterns after tumor resection and high-dose proton boost
Abstract
Background: Glioblastoma peritumoral edema (PE) extent is associated with survival and progression pattern after tumor resection and radiotherapy (RT). To increase tumor control, proton beam was adopted to give high-dose boost (> 90 Gy). However, the correlation between PE extent and prognosis of glioblastoma after postoperative high-dose proton boost (HDPB) therapy stays unknown. We intend to utilize the PE status to classify the survival and progression patterns.
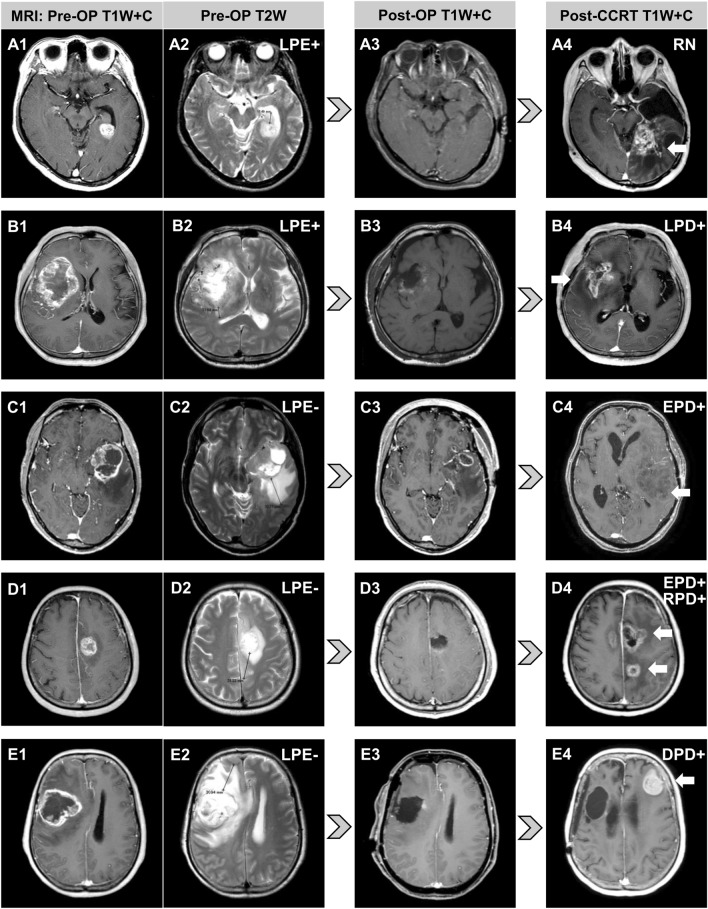
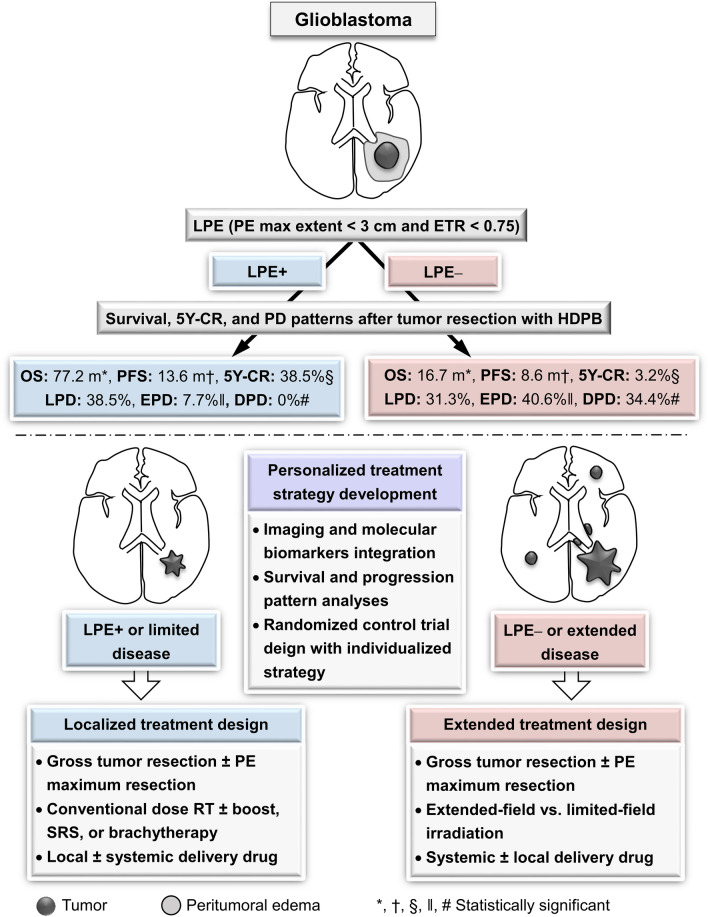
Methods: Patients receiving HDPB (96.6 GyE) were retrospectively evaluated. Limited peritumoral edema (LPE) was defined as PE extent < 3 cm with a ratio of PE extent to tumor maximum diameter of < 0.75. Extended progressive disease (EPD) was defined as progression of tumors extending > 1 cm from the tumor bed edge.
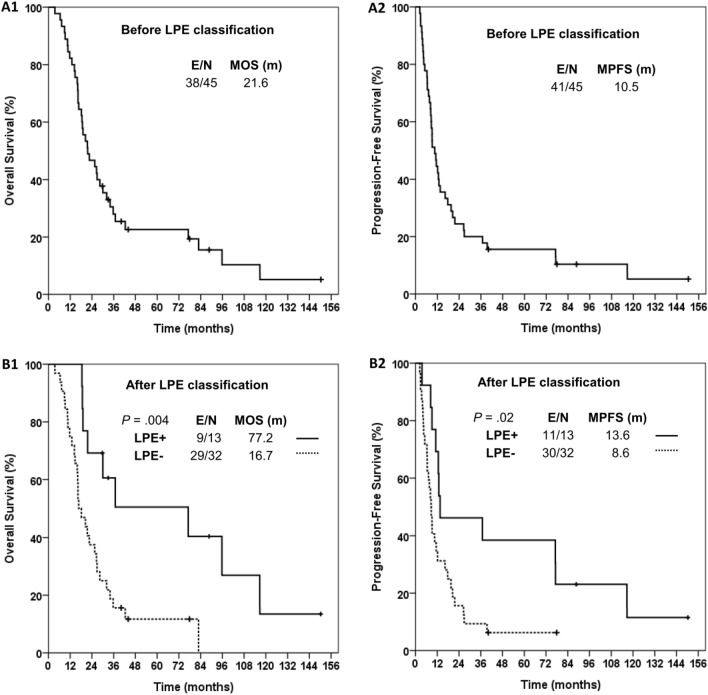
Results: After long-term follow-up (median 88.7, range 63.6-113.8 months) for surviving patients with (n = 13) and without (n = 32) LPE, the median overall survival (OS) and progression-free survival (PFS) were 77.2 vs. 16.7 months (p = 0.004) and 13.6 vs. 8.6 months (p = 0.02), respectively. In multivariate analyses combined with factors of performance, age, tumor maximum diameter, and tumor resection extent, LPE remained a significant factor for favorable OS and PFS. The rates of 5-year complete response, EPD, and distant metastasis with and without LPE were 38.5% vs. 3.2% (p = 0.005), 7.7% vs. 40.6% (p = 0.04), and 0% vs. 34.4% (p = 0.02), respectively.
Conclusions: The LPE status effectively identified patients with relative long-term control and specific progression patterns after postoperative HDPB for glioblastoma.
Keywords: Dose-escalated radiotherapy; Glioblastoma; Imaging biomarker; Peritumoral edema; Personalized treatment; Proton beam therapy.
© 2021. The Author(s).
Conflict of interest statement
No competing interests.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
