

Coffee break has no impact on laparoscopic skills: a randomized double-blinded placebo-controlled parallel-group trial
- PMID: 34459976
- PMCID: PMC9001621
- DOI: 10.1007/s00464-021-08675-9
Coffee break has no impact on laparoscopic skills: a randomized double-blinded placebo-controlled parallel-group trial
Abstract
Background: Coffee is a widely consumed beverage. Surgeons often drink coffee before performing surgery. Caffeine intake leads to tremor which might have a negative effect on surgeons' fine motor skills.
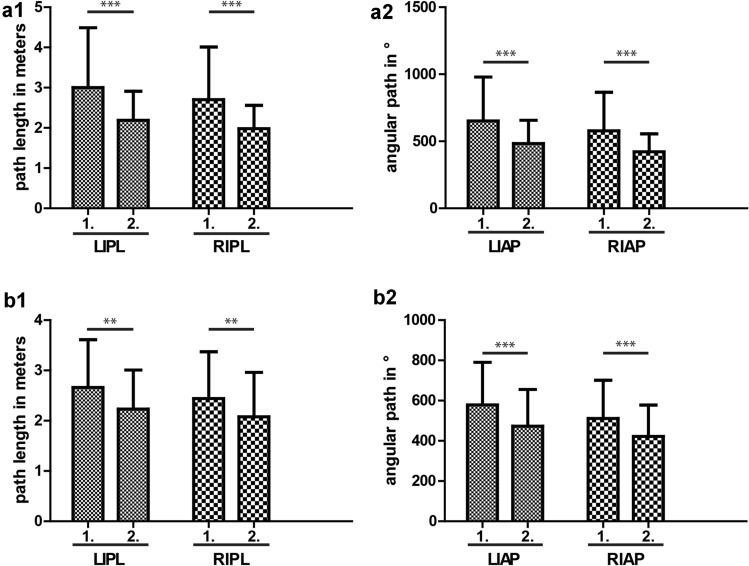
Methods: A double-blinded parallel-group trial was conducted in order to investigate if caffeinated coffee intake has a negative effect on laparoscopic skills and increases tremor, regardless of previous coffee consumption. 118 participants were selected during a congress of the German Society of Surgery. Exclusion criteria were immaturity and no given consent. Participants and investigators were blinded. Participants were randomized with a 1:1 allocation into interventional group receiving caffeinated coffee or placebo group receiving decaffeinated coffee. The motor skills were tested with two validated laparoscopic exercises at a laparoscopy simulator (LapSim®) before and 30 min after coffee intake. Data on influencing factors were recorded in a standardized questionnaire and tested for equal distribution in both groups. In both exercises four parameters were recorded: left and right hand path length and angular path. Their differences and the resulting effect scores were calculated for both groups as primary outcome to test which group showed greater improvement on the second round of exercises. Registration number DRKS00023608, registered retrospectively.
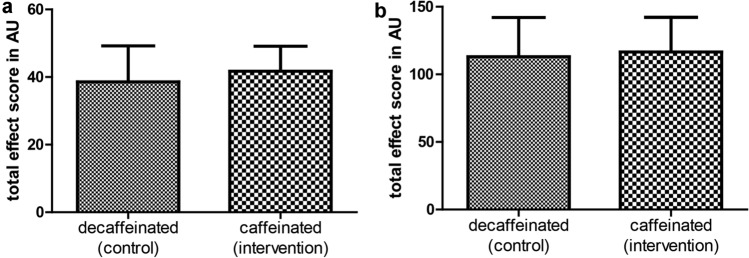
Results: Fifty nine subjects were assigned to each the interventional (54 analyzed) and placebo group (53 analyzed) with 11 drop outs. There was no significant difference between the placebo and interventional group in the two exercises in effect score 30 min after coffee intake [mean (SD); 38.58 (10.66) vs. 41.73 (7.40) and 113.09 (28.94) vs. 116.59 (25.63)]. A significant improvement from first to second measurement in the first exercise could be observed for both groups, demonstrating the training effect.
Conclusion: In our study, we verified that additional caffeinated coffee intake, e.g., during a coffee break, does not lead to deterioration of laparoscopic fine motor skills.
Keywords: Caffeine; Coffee; Fine motor skills; Laparoscopy; Surgery; Tremor.
© 2021. The Author(s).
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
