

Age-stratified and blood-pressure-stratified effects of blood-pressure-lowering pharmacotherapy for the prevention of cardiovascular disease and death: an individual participant-level data meta-analysis
- PMID: 34461040
- PMCID: PMC8473559
- DOI: 10.1016/S0140-6736(21)01921-8
Age-stratified and blood-pressure-stratified effects of blood-pressure-lowering pharmacotherapy for the prevention of cardiovascular disease and death: an individual participant-level data meta-analysis
Abstract
Background: The effects of pharmacological blood-pressure-lowering on cardiovascular outcomes in individuals aged 70 years and older, particularly when blood pressure is not substantially increased, is uncertain. We compared the effects of blood-pressure-lowering treatment on the risk of major cardiovascular events in groups of patients stratified by age and blood pressure at baseline.
Methods: We did a meta-analysis using individual participant-level data from randomised controlled trials of pharmacological blood-pressure-lowering versus placebo or other classes of blood-pressure-lowering medications, or between more versus less intensive treatment strategies, which had at least 1000 persons-years of follow-up in each treatment group. Participants with previous history of heart failure were excluded. Data were obtained from the Blood Pressure Lowering Treatment Triallists' Collaboration. We pooled the data and categorised participants into baseline age groups (<55 years, 55-64 years, 65-74 years, 75-84 years, and ≥85 years) and blood pressure categories (in 10 mm Hg increments from <120 mm Hg to ≥170 mm Hg systolic blood pressure and from <70 mm Hg to ≥110 mm Hg diastolic). We used a fixed effects one-stage approach and applied Cox proportional hazard models, stratified by trial, to analyse the data. The primary outcome was defined as either a composite of fatal or non-fatal stroke, fatal or non-fatal myocardial infarction or ischaemic heart disease, or heart failure causing death or requiring hospital admission.
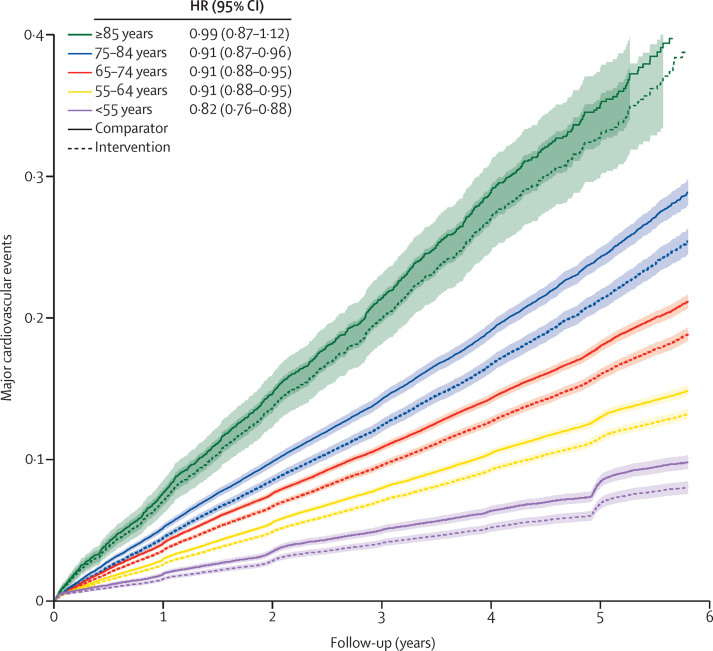
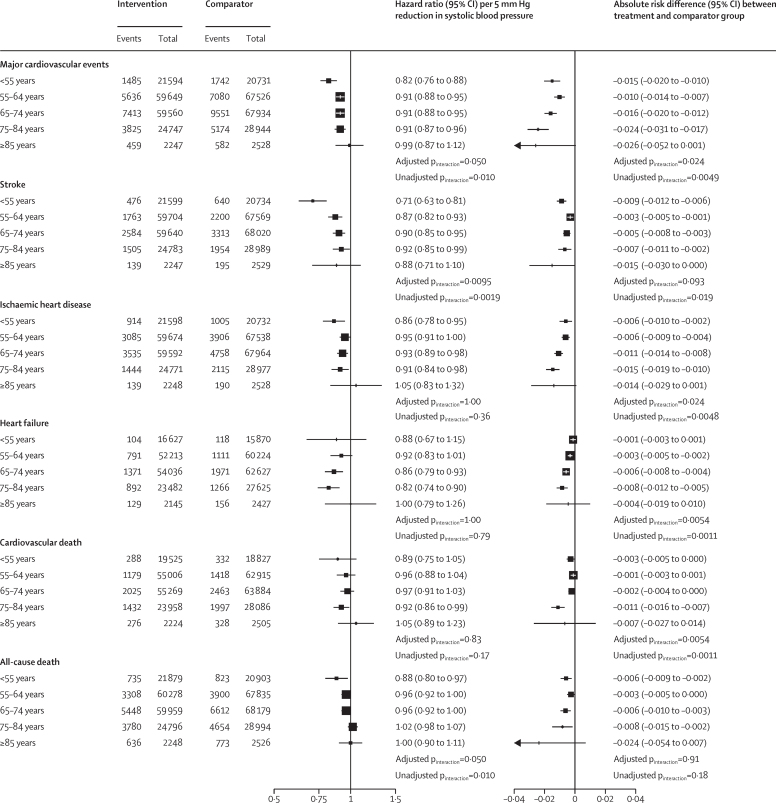
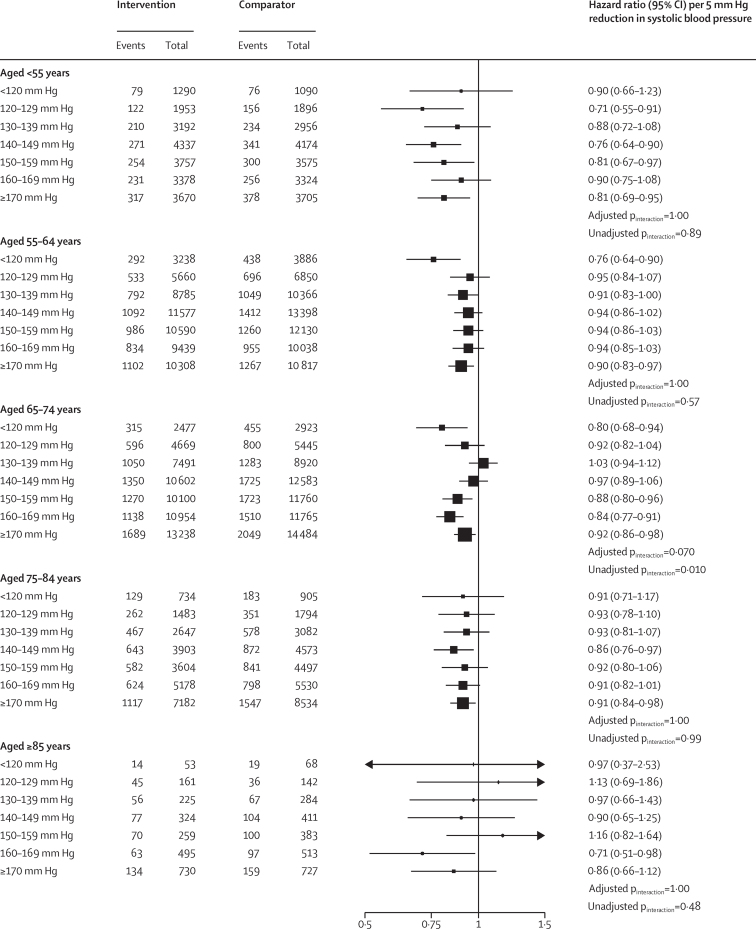
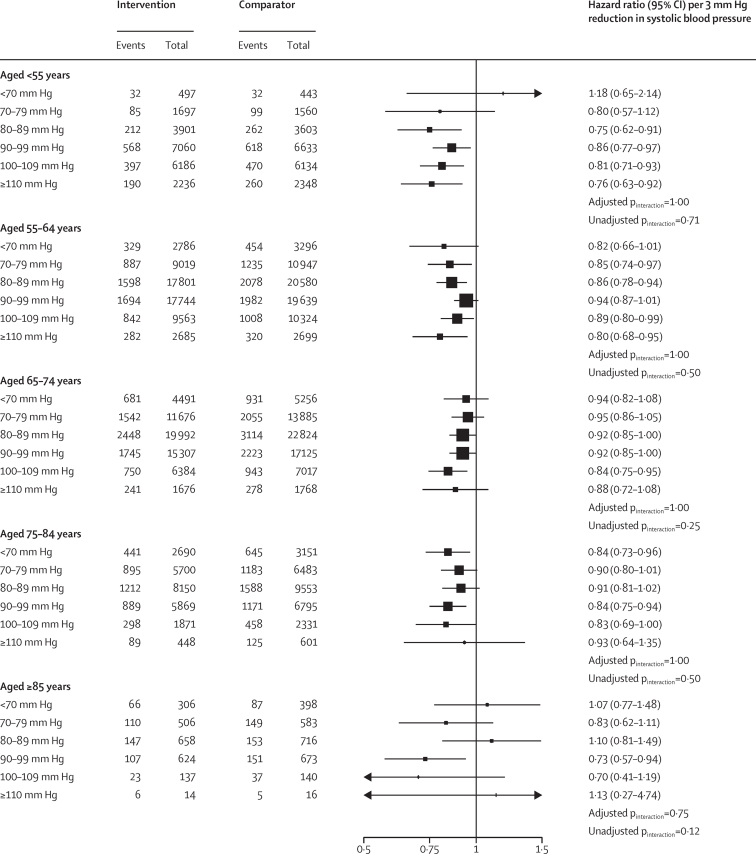
Findings: We included data from 358 707 participants from 51 randomised clinical trials. The age of participants at randomisation ranged from 21 years to 105 years (median 65 years [IQR 59-75]), with 42 960 (12·0%) participants younger than 55 years, 128 437 (35·8%) aged 55-64 years, 128 506 (35·8%) 65-74 years, 54 016 (15·1%) 75-84 years, and 4788 (1·3%) 85 years and older. The hazard ratios for the risk of major cardiovascular events per 5 mm Hg reduction in systolic blood pressure for each age group were 0·82 (95% CI 0·76-0·88) in individuals younger than 55 years, 0·91 (0·88-0·95) in those aged 55-64 years, 0·91 (0·88-0·95) in those aged 65-74 years, 0·91 (0·87-0·96) in those aged 75-84 years, and 0·99 (0·87-1·12) in those aged 85 years and older (adjusted pinteraction=0·050). Similar patterns of proportional risk reductions were observed for a 3 mm Hg reduction in diastolic blood pressure. Absolute risk reductions for major cardiovascular events varied by age and were larger in older groups (adjusted pinteraction=0·024). We did not find evidence for any clinically meaningful heterogeneity of relative treatment effects across different baseline blood pressure categories in any age group.
Interpretation: Pharmacological blood pressure reduction is effective into old age, with no evidence that relative risk reductions for prevention of major cardiovascular events vary by systolic or diastolic blood pressure levels at randomisation, down to less than 120/70 mm Hg. Pharmacological blood pressure reduction should, therefore, be considered an important treatment option regardless of age, with the removal of age-related blood-pressure thresholds from international guidelines.
Funding: British Heart Foundation, National Institute of Health Research Oxford Biomedical Research Centre, Oxford Martin School.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MN reports grants from the British Heart Foundation, outside the submitted work. DC reports grants from the British Heart Foundation, during the conduct of the study. KR reports grants from the British Heart Foundation, the UK Research and Innovation Global Challenges Research Fund, Oxford Martin School, University of Oxford, and NIHR Oxford Biomedical Research Centre, University of Oxford, during the conduct of the study; personal fees from Heart, outside the submitted work; and research support and consulting fees to the University by Medtronic. JC reports grants from the National Health and Medical Research Council of Australia, outside the submitted work. CJP has recived grants from the US National Institutes of Health/National Heart, Lung and Blood Institute, BioCardia, GE Health Care, Caladrius Biosciences, Merck, Sanofi, CSL Behring, XyloCor Therapeutics, Mesoblast, Ventrix, and Athersys. All other authors declare no competing interests.
Figures
Comment in
-
Time to remove hypertension from our vocabulary?Lancet. 2021 Sep 18;398(10305):1023-1025. doi: 10.1016/S0140-6736(21)01916-4. Epub 2021 Aug 27. Lancet. 2021. PMID: 34461041 No abstract available.
-
Intensive blood pressure control benefits older patients.Nat Rev Cardiol. 2021 Nov;18(11):739. doi: 10.1038/s41569-021-00626-0. Nat Rev Cardiol. 2021. PMID: 34526678 No abstract available.
-
Age-independent benefits of blood pressure lowering: are they applicable to all patients?Eur Heart J. 2022 Feb 10;43(6):448-449. doi: 10.1093/eurheartj/ehab825. Eur Heart J. 2022. PMID: 35143651 No abstract available.
-
Blood pressure meta-analysis highlights an implementation gap.Lancet. 2022 Apr 9;399(10333):1379-1380. doi: 10.1016/S0140-6736(22)00192-1. Lancet. 2022. PMID: 35397861 No abstract available.
References
-
- Ettehad D, Emdin CA, Kiran A. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–967. - PubMed
-
- Pinho-Gomes A-C, Rahimi K. Blood pressure management in the elderly: the need for more randomised evidence. Heart. 2019;105:1055–1056. - PubMed
-
- Rahimi K, Emdin CA, MacMahon S. The epidemiology of blood pressure and its worldwide management. Circ Res. 2015;116:925–936. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
