

Explosive nosocomial outbreak of SARS-CoV-2 in a rehabilitation clinic: the limits of genomics for outbreak reconstruction
- PMID: 34461177
- PMCID: PMC8393517
- DOI: 10.1016/j.jhin.2021.07.013
Explosive nosocomial outbreak of SARS-CoV-2 in a rehabilitation clinic: the limits of genomics for outbreak reconstruction
Abstract
Background: Nosocomial outbreaks of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) are frequent despite implementation of conventional infection control measures. An outbreak investigation was undertaken using advanced genomic and statistical techniques to reconstruct likely transmission chains and assess the role of healthcare workers (HCWs) in SARS-CoV-2 transmission.
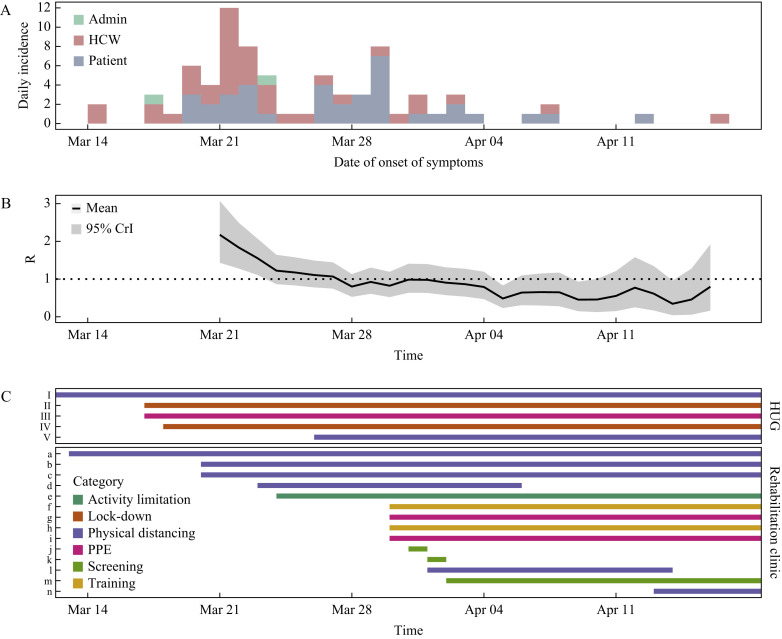
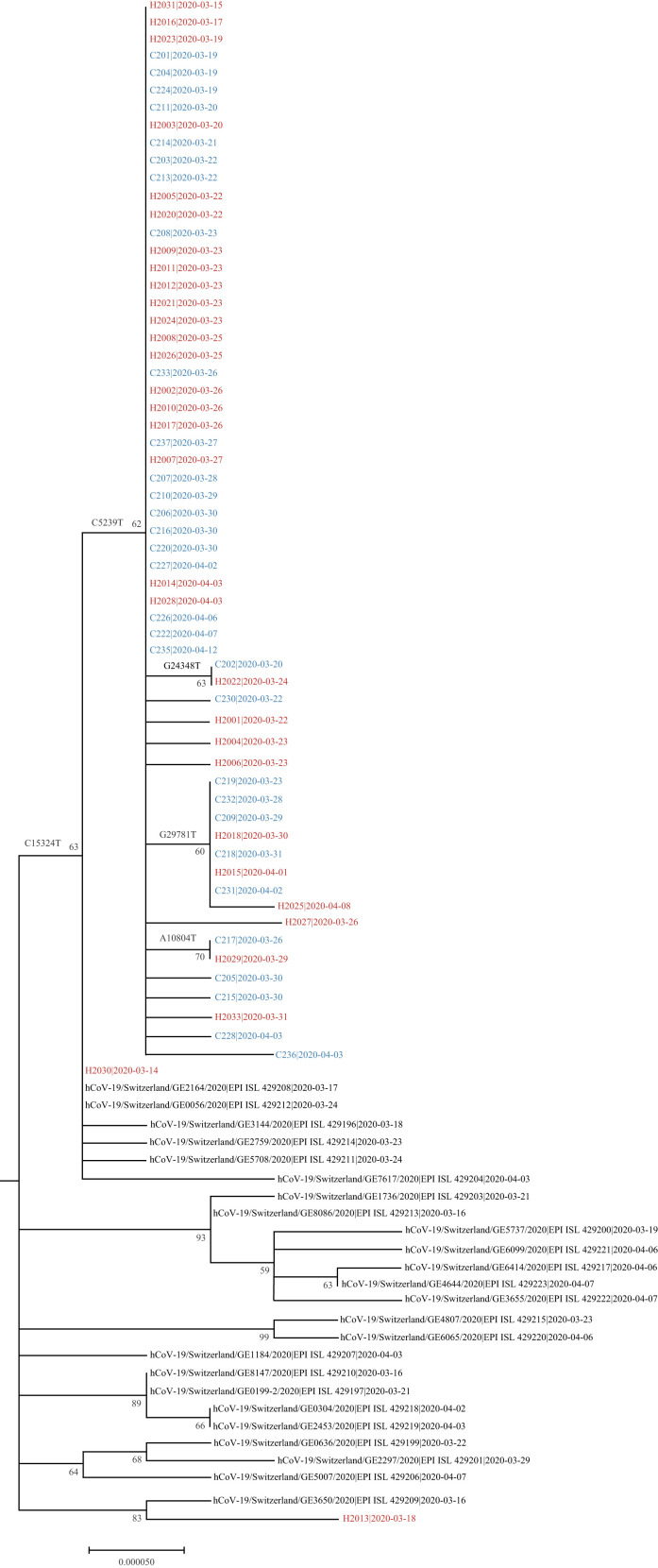
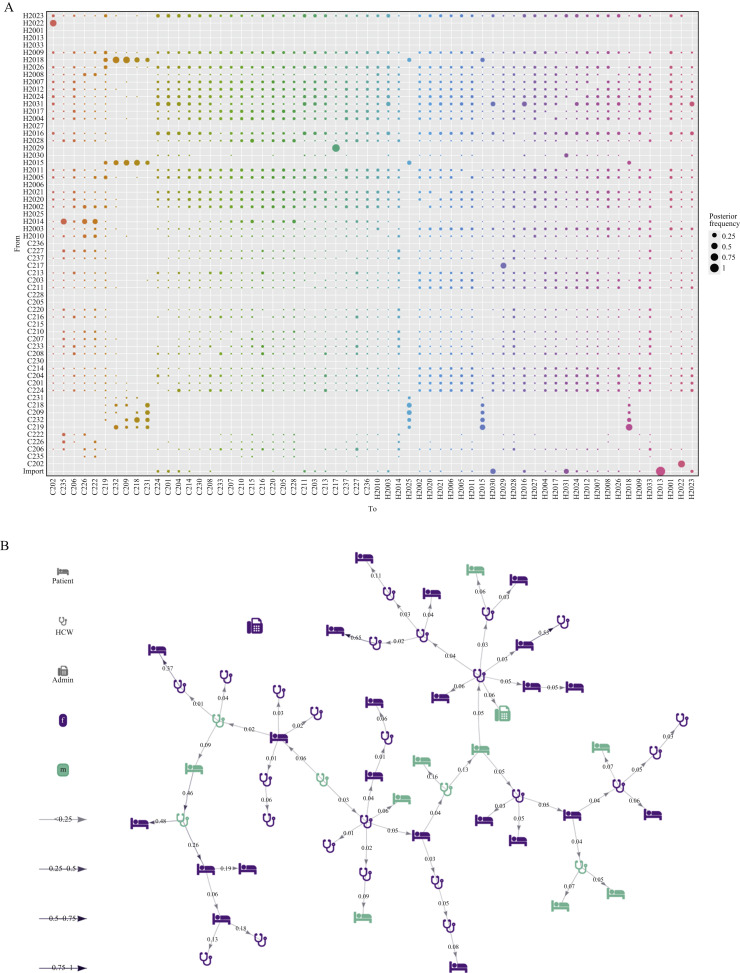
Methods: A nosocomial SARS-CoV-2 outbreak in a university-affiliated rehabilitation clinic was investigated, involving patients and HCWs, with high coverage of pathogen whole-genome sequences (WGS). The time-varying reproduction number from epidemiological data (Rt) was estimated, and maximum likelihood phylogeny was used to assess genetic diversity of the pathogen. Genomic and epidemiological data were combined into a Bayesian framework to model the directionality of transmission, and a case-control study was performed to investigate risk factors for nosocomial SARS-CoV-2 acquisition in patients.
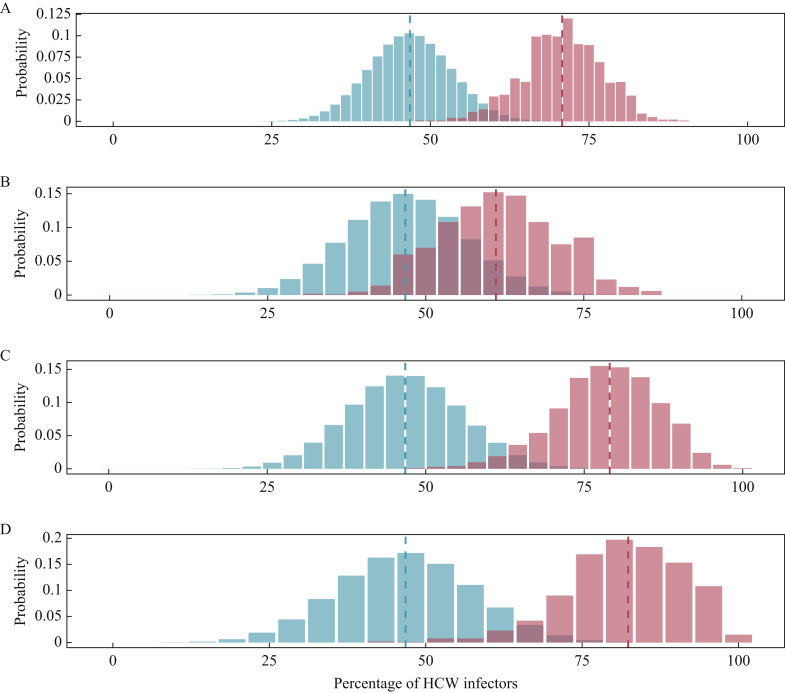
Findings: The outbreak lasted from 14th March to 12th April 2020, and involved 37 patients (31 with WGS) and 39 employees (31 with WGS), 37 of whom were HCWs. Peak Rt was estimated to be between 2.2 and 3.6. The phylogenetic tree showed very limited genetic diversity, with 60 of 62 (96.7%) isolates forming one large cluster of identical genomes. Despite the resulting uncertainty in reconstructed transmission events, the analyses suggest that HCWs (one of whom was the index case) played an essential role in cross-transmission, with a significantly greater fraction of infections (P<2.2e-16) attributable to HCWs (70.7%) than expected given the number of HCW cases (46.7%). The excess of transmission from HCWs was higher when considering infection of patients [79.0%; 95% confidence interval (CI) 78.5-79.5%] and frail patients (Clinical Frailty Scale score >5; 82.3%; 95% CI 81.8-83.4%). Furthermore, frail patients were found to be at greater risk for nosocomial COVID-19 than other patients (adjusted odds ratio 6.94, 95% CI 2.13-22.57).
Interpretation: This outbreak report highlights the essential role of HCWs in SARS-CoV-2 transmission dynamics in healthcare settings. Limited genetic diversity in pathogen genomes hampered the reconstruction of individual transmission events, resulting in substantial uncertainty in who infected whom. However, this study shows that despite such uncertainty, significant transmission patterns can be observed.
Keywords: COVID-19; Healthcare-associated infection; Infection prevention and control; Long-term care facilities; Nosocomial outbreaks; SARS-CoV-2.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
