

Artemisinin-based combination therapy for uncomplicated Plasmodium falciparum malaria in Mali: a systematic review and meta-analysis
- PMID: 34461901
- PMCID: PMC8404312
- DOI: 10.1186/s12936-021-03890-0
Artemisinin-based combination therapy for uncomplicated Plasmodium falciparum malaria in Mali: a systematic review and meta-analysis
Abstract
Background: Artemisinin-based combination therapy (ACT) was deployed in 2005 as an alternative to chloroquine and is considered the most efficacious treatment currently available for uncomplicated falciparum malaria. While widespread artemisinin resistance has not been reported to date in Africa, recent studies have reported partial resistance in Rwanda. The purpose of this study is to provide a current systematic review and meta-analysis on ACT at Mali study sites, where falciparum malaria is highly endemic.
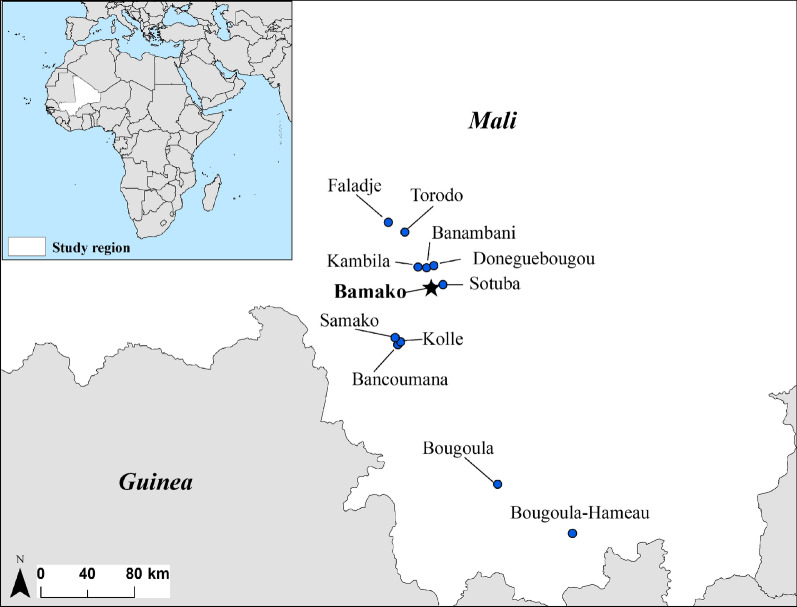
Methods: A systematic review of the literature maintained in the bibliographic databases accessible through the PubMed, ScienceDirect and Web of Science search engines was performed to identify research studies on ACT occurring at Mali study sites. Selected studies included trials occurring at Mali study sites with reported polymerase chain reaction (PCR)-corrected adequate clinical and parasite response rates (ACPRcs) at 28 days. Data were stratified by treatment arm (artemether-lumefantrine (AL), the first-line treatment for falciparum malaria in Mali and non-AL arms) and analysed using random-effects, meta-analysis approaches.
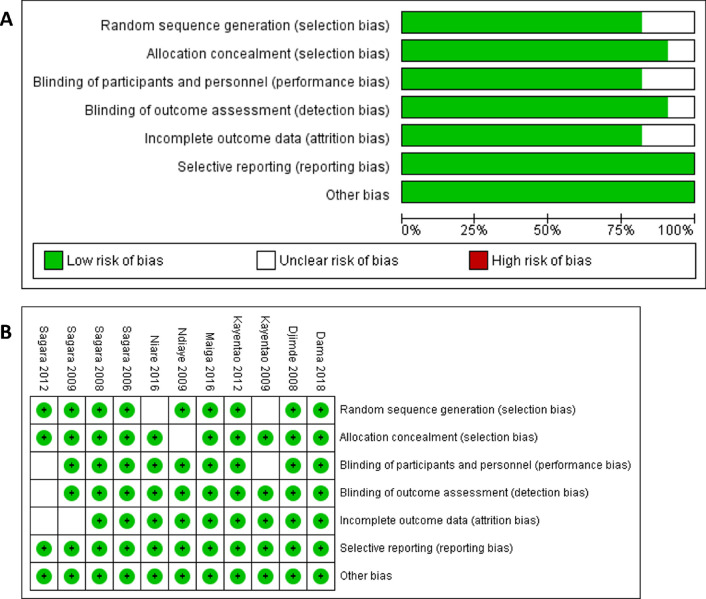
Results: A total of 11 studies met the inclusion criteria, and a risk of bias assessment carried out by two independent reviewers determined low risk of bias among all assessed criteria. The ACPRc for the first-line AL at Mali sites was 99.0% (95% CI (98.3%, 99.8%)), while the ACPRc among non-AL treatment arms was 98.9% (95% CI (98.3%, 99.5%)). The difference in ACPRcs between non-AL treatment arms and AL treatment arms was not statistically significant (p = .752), suggesting that there are potential treatment alternatives beyond the first-line of AL in Mali.
Conclusions: ACT remains highly efficacious in treating uncomplicated falciparum malaria in Mali. Country-specific meta-analyses on ACT are needed on an ongoing basis for monitoring and evaluating drug efficacy patterns to guide local malaria treatment policies, particularly in the wake of observed artemisinin resistance in Southeast Asia and partial resistance in Rwanda.
Keywords: Artemether–lumefantrine; Artemisinin-based combination therapy; Malaria; Mali; Systematic review.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- WHO. Malaria: key facts. Geneva, World Health Organization, 2020. https://www.who.int/news-room/fact-sheets/detail/malaria.
-
- WHO. World Malaria Report 2018. Geneva, World Health Organization, 2018. https://www.who.int/malaria/publications/world-malaria-report-2018/en/.
-
- Diallo MA, Yade MS, Ndiaye YD, Diallo I, Diongue K, Sy SA, et al. Efficacy and safety of artemisinin-based combination therapy and the implications of Pfkelch13 and Pfcoronin molecular markers in treatment failure in Senegal. Sci Rep. 2020;10:8907. doi: 10.1038/s41598-020-65553-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
