

Congenital hepatic fibrosis and its mimics: a clinicopathologic study of 19 cases at a single institution
- PMID: 34461951
- PMCID: PMC8406726
- DOI: 10.1186/s13000-021-01142-y
Congenital hepatic fibrosis and its mimics: a clinicopathologic study of 19 cases at a single institution
Abstract
Background: Congenital hepatic fibrosis (CHF) is a rare inherited form of ductal plate malformation associated with polycystic kidney disease. The diagnosis requires histopathologic confirmation, but can be challenging to distinguish from other undefined fibrocystic liver diseases. We aimed to describe the clinicopathologic features of congenital hepatic fibrosis (CHF), with comparisons to other entities that may clinically and/or histologically mimic CHF.
Methods: Nineteen cases that carried a clinical and/or histologic impression of CHF were identified at our institution, of which the histology was reassessed and reappraised into two categories: CHF (n=13) and mimics (n=6). The clinicopathologic features between the two groups were analyzed and compared.
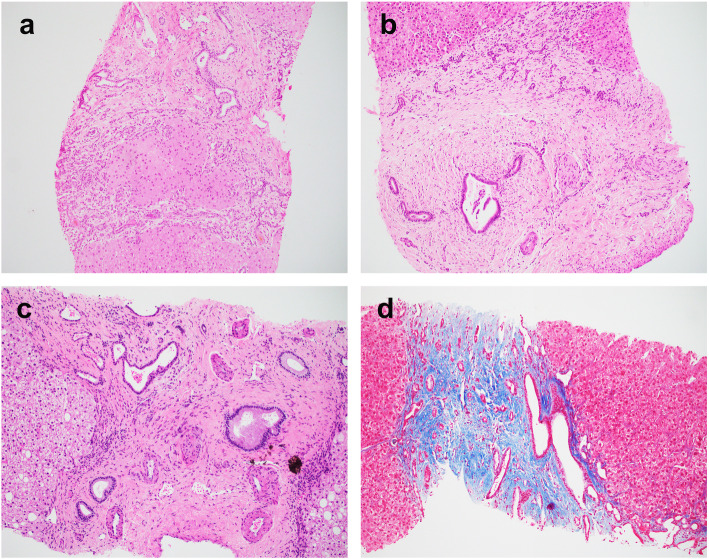
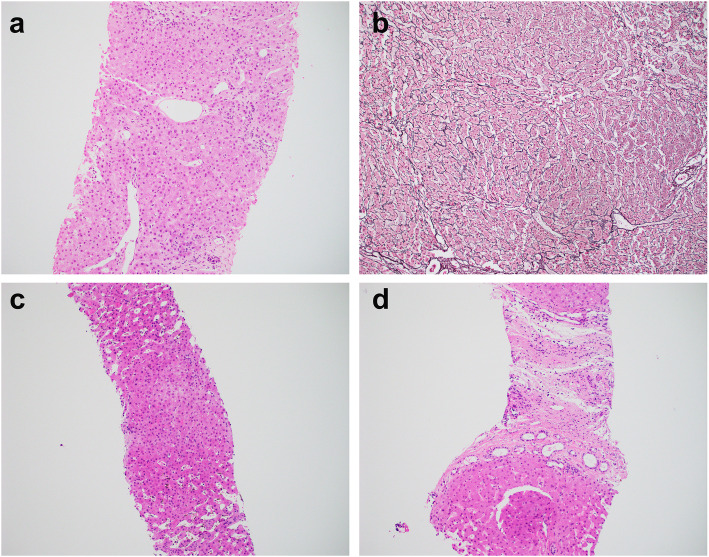
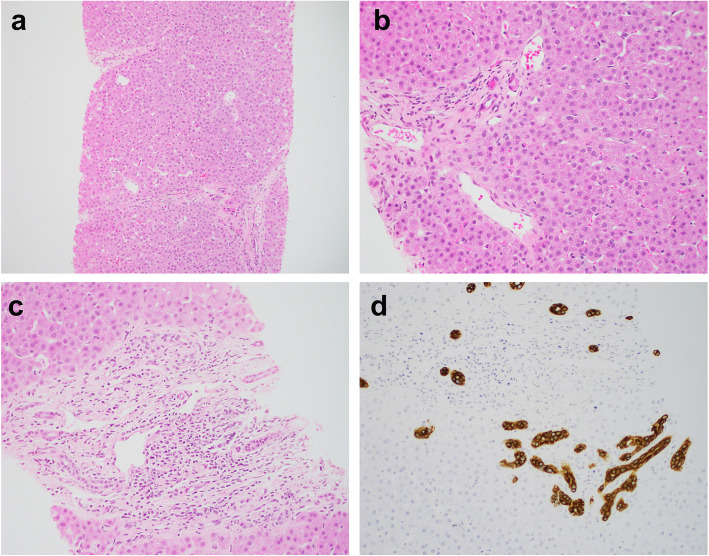
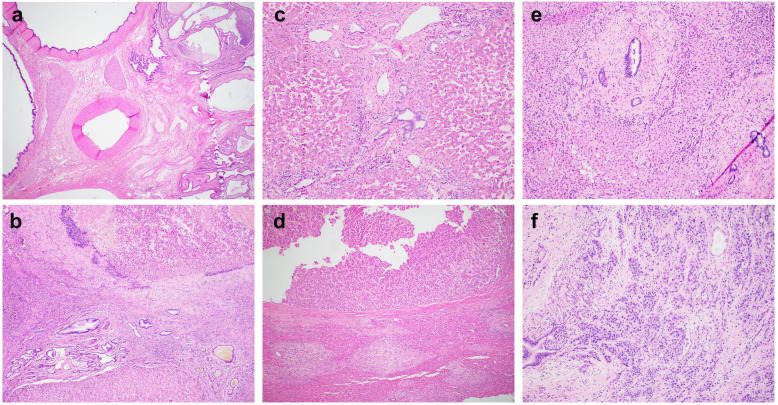
Results: The CHF group was further sub-classified into those with clinical suspicion (CHF-c, n=8) and those as incidental histology findings (CHF-i, n=5). Patients of CHF-i were much older than CHF-c or mimics (P<0.05). Male and female were equally affected. Six of 8 CHF-c (66.7%) had concurrent kidney diseases, including 5 polycystic kidney diseases. Five of 6 mimics (83.3%) had various kidney diseases, including nephronophthisis, Alport syndrome, renal agenesis, and nephrolithiasis. None of the CHF-i patients had kidney disease, but 3 were associated with hepatic carcinomas. Histology analysis demonstrated characteristic triads (bile duct abnormalities, portal vein hypoplasia, and fibrosis) in all CHF cases. One mimic had paucity of intrahepatic bile ducts, while the other 5 mimics showed abnormal portal veins and nodular regenerative hyperplasia consistent with hepatoportal sclerosis (HPS).
Conclusions: Our study demonstrates classic histology triad of CHF despite a wide spectrum of clinical presentations. HPS is unexpectedly a clinical mimicker of CHF, which can be distinguished histologically.
Keywords: Congenital hepatic fibrosis; Hepatoportal sclerosis; Nodular regenerative hyperplasia; Portal hypertension.
© 2021. The Author(s).
Conflict of interest statement
None.
Figures
References
-
- Saxena R. Practical hepatic pathology: A diagnostic approach. 2nd Ed. Philadelphia: Elsevier; 2018.
-
- Redston MS, Wanless IR. The hepatic von Meyenburg complex: prevalence and association with hepatic and renal cysts among 2843 autopsies [corrected] Mod Pathol. 1996;9(3):233–237. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
