

Evaluation of inter- and intra-fraction 6D motion for stereotactic body radiation therapy of spinal metastases: influence of treatment time
- PMID: 34461953
- PMCID: PMC8404277
- DOI: 10.1186/s13014-021-01892-5
Evaluation of inter- and intra-fraction 6D motion for stereotactic body radiation therapy of spinal metastases: influence of treatment time
Abstract
Background: The objective of this study was to analyze the amplitude of translational and rotational movements occurring during stereotactic body radiotherapy (SBRT) of spinal metastases in two different positioning devices. The relevance of intra-fractional imaging and the influence of treatment time were evaluated.
Methods: Twenty patients were treated in the supine position either (1) on a body vacuum cushion with arms raised and resting on a clegecel or (2) on an integrated SBRT solution consisting of a SBRT table top, an Orfit™ AIO system, and a vacuum cushion. Alignments between the cone beam computed tomography (CBCT) and the planning computed tomography allowed corrections of inter- and intra-fraction positional shifts using a 6D table. The absolute values of the translational and rotational setup errors obtained for 329 CBCT were recorded. The translational 3D vector, the maximum angle, and the characteristic times of the treatment fractions were calculated.
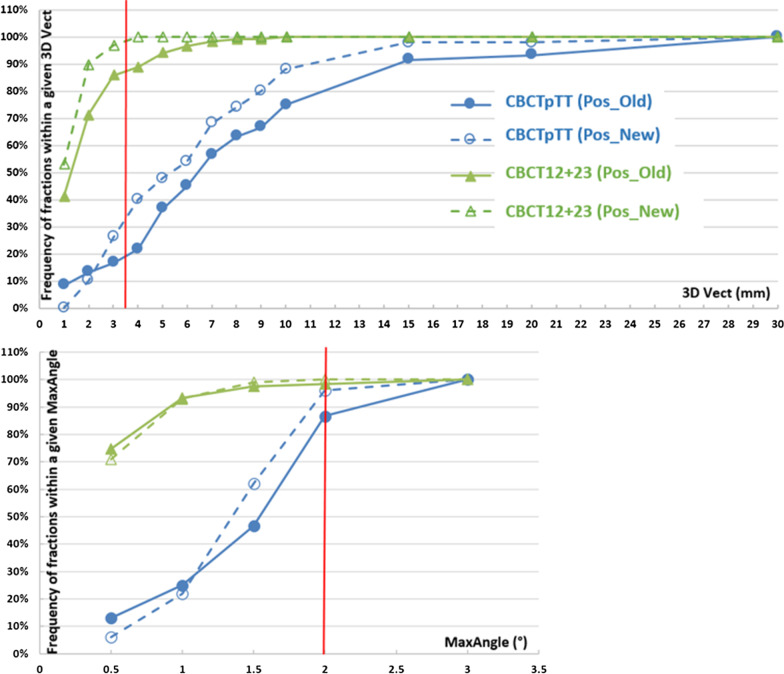
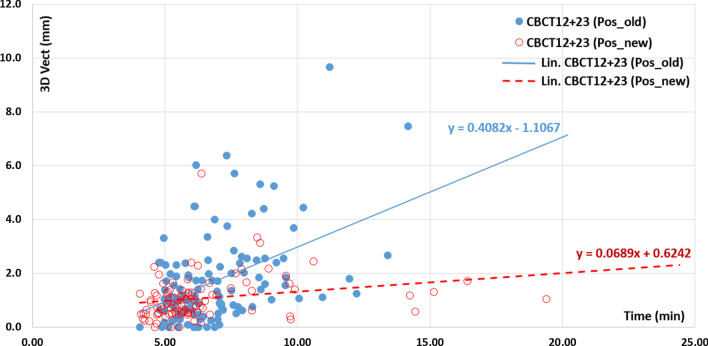
Results: An improvement in the mean (SD) inter-fraction 3D vector (mm) from 7.8 (5.9) to 5.9 (3.8) was obtained by changing the fixation devices from (1) to (2) (p < 0.038). The maximum angles were less than 2° for a total of 87% for (1) and 96% for (2). The mean (SD) of the intra-fraction 3D vectors (mm) was lower for the new 1.1 (0.8) positioning fixation (2) compared to the old one (1) 1.7 (1.7) (p = 0.004). The angular corrections applied in the intra-fraction were on average very low (0.4°) and similar between the two systems. A strong correlation was found between the 3D displacement vector and the fraction time for (1) and (2) with regression coefficients of 0.408 (0.262-0.555, 95% CI) and 0.069 (0.010-0.128, 95% CI), respectively. An accuracy of 1 mm would require intra-fraction imaging every 5 min for both systems. If the expected accuracy was 2 mm, then only system (2) could avoid intra-fractional imaging.
Conclusions: This study allowed us to evaluate setup errors of two immobilization devices for spine SBRT. The association of inter- and intra-fraction imaging with 6D repositioning of a patient is inevitable. The correlation between treatment time and corrections to be applied encourages us to move toward imaging modalities which allow a reduction in fraction time.
Keywords: CBCT; Inter-fraction; Intra-fraction; SBRT; Spinal; Treatment time.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Khan M, Ambady P, Kimbrough D, Shoemaker T, Terezakis S, Blakeley J, et al. Radiation-induced myelitis: initial and follow-up MRI and clinical features in patients at a single tertiary care institution during 20 years. Am J Neuroradiol. 2018;39:1576–1581. doi: 10.3174/ajnr.A5680. - DOI - PMC - PubMed
-
- Lee J et al. Stereotactic ablative body radiation therapy (SABR): a resource SABR UK consortium. Endorsed by The Faculty of Clinical Oncology of the Royal College of Radiologists. Version 6.1, January 2019
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
